Exploring Parent/Caregiver Perspectives of Self-Determination and Its Impact on Mental Health in Adolescents With and Without Disabilities
Jessica Oeth Schuttler; Sydney Walls; Tyler Hicks; Karrie A. Shogren; Hannah Adams; and Richard A. Chapman
Schuttler, J. O., Walls, S., Hicks, T., Shogren, K. A., Adams, H., & Chapman, R. A. (2024). Exploring parent/caregiver perspectives of self-determination and its impact on mental health in adolescents with and without disabilities. Developmental Disabilities Network Journal, 4(1), 15-32.
Plain Language Summary
Self-determination is the idea of making things happen in your life. Mental health is the idea of taking care of your mind, your ideas, and your feelings. Parents can help teens grow in their self-determination. Parents can also help teens with their mental health. We need to understand this better for teens with disabilities.
In this project, we wanted to learn how parents see mental health and self-determination for teens in their family. We also wanted to learn how mental health symptoms and self-determination might be different for different teens. We asked teens and their parents to be part of our project. We asked teens of different genders to be in the study. We also asked teens who had disabilities and teens who did not have disabilities to be in the study. In this paper we will talk about what parents thought. In a future paper we will talk about what we learned from the teens.
Parents filled out two questionnaires. One was about how parents saw their teens show self-determination. One was about how teens show mental health symptoms. We looked at parent responses using statistics. Parents reported that self-determination affects how teens feel and show stress. Self-determination is related to mood and attention. Parents said self-determination impacted how teens shared strong feelings. Self-determination is also related to teens’ daily living skills. These impacts were different for different teens. They could be different for teens of different genders. They could also be different for teens with or without disabilities.
This is a new study. Only a small group of people were in the study. We need to ask more people to tell us how they feel. We want to find out more about other kinds of support teens have—like friends, school, or jobs. Then we can better understand teens’ mental health and self-determination. We will keep studying these ideas in the future. It is important to support self-determination and mental health for all teens.
Abstract
Parents and caregivers play key roles in supporting the development of self-determination and mental health needs in adolescents with and without disabilities. This study explored parent/caregiver perceptions of the relationships among mental health and self-determination constructs for youth with disabilities, across gender and disability status. Parents/caregivers of adolescents with and without disabilities completed rating scales regarding adolescents’ self-determination status (Self Determination Inventory) and mental health symptoms (Behavior Assessment System for Children, 3rd Edition). Bayesian analyses examined the relationships between self-determination and mental health status. Results are mixed, indicating moderate to robust relationships for self-determination as a moderator for the relationship between disability status and adaptive skills and behavioral symptoms, but mixed results for self-determination as a moderator of those demographic variables on internalizing and externalizing symptoms. While sample size is limited, results suggest that there are potential relationships among these variables that warrant further exploration.
Introduction
The importance of agency and self-determined actions have a long history in the disability field. Over 50 years of research have refined our understanding of self-determination to emphasize the critical role of action and causal agency across the lifespan and the need for opportunities to cultivate self-determination characteristics in childhood, adolescence, and adulthood (Shogren & Raley, 2022). Causal Agency Theory (Shogren & Raley, 2022, p. 33) describes “how” people become self-determined within their respective contexts and refines the definition of self-determination as a “dispositional characteristic manifested as acting as the causal agent in one’s life” (Shogren et al., 2015, p. 258). Causal Agency Theory integrates aspects of Self-Determination Theory (Deci & Ryan, 2012), a psychological theory of motivation that defines the constructs of autonomy, relatedness, and competence as key psychological needs for an individual that drive human actions. Causal Agency Theory encompasses the notions of (1) building people’s personal capacities (skills and abilities) for self-determined actions (e.g., choice making, goal setting, decision making), (2) enhancing environmental supports to create opportunities for self-determined actions (e.g., supporting people’s basic psychological needs and providing opportunities for expressions of self-determination), and (3) establishing personalized and systematic supports for people within their chosen contexts (Shogren & Raley, 2022, p. 31).
As a theory of human agency, Causal Agency Theory relates closely to other definitions/ conceptualizations of human functioning and recognizes the reciprocal relationship between a person and their contexts and the role of beliefs in shaping interactions across contexts. As Little et al. (2006) theorize, humans come into various states of dysfunction when they encounter a challenge with inadequate beliefs about their agency to reach a goal (either how they attribute their abilities in addressing a threat or capitalizing on an opportunity to move towards that goal), leading to emotional dysregulation such as anxiety, depression, or other disorders. Within the psychotherapeutic relationship, consideration of (and support for) the development of agency is an important, albeit under-researched, feature of work between a therapist and a client.
When considering the interplay of mental health and disability, the positive psychology construct of self-regulation—the capacity to gauge one’s presence in a situation and regulate oneself to maintain and successfully navigate various environments and expectations—is compelling to consider (Diamond & Aspinwall, 2003; Shogren et al., 2006). Challenges with self-regulation can manifest as difficulties with managing both internalizing (e.g., anxiety, negative mood, distractibility) and externalizing (e.g., aggression, impulsivity, disruptive behavior) symptoms, which, without support, can lead to ongoing mental health problems limiting self-determination and agency. Measurement of self-regulation and problems with self-regulation can include screening measures such as the Achenbach Child Behavior Checklist (CBCL) or the Behavior Assessment System for Children, 3rd Edition (BASC-3).
The trajectory of social-emotional development for youth with disabilities can be impacted by environmental barriers and challenges to causal agency leading to increased stress and anxiety. Psychological distress and serious mental illness are more prevalent in disabled populations as opposed to non-disabled populations, with the highest prevalence in those with cognitive disabilities (Lauer & Lauer, 2019). Studies have suggested that individuals with autism and intellectual disability (ID) are at heightened risk for co-occurring mental health conditions, such as anxiety and depression, compared to peers without disabilities (DeFillipis, 2018; Van Steensel et al., 2011). A contributing factor to this increased risk can be a lack of environmental supports and protective factors (such as family support for self-determination), as well as social support networks outside of the family, in comparison to nondisabled peers. Thus, for many youth with disabilities, we see higher prevalence rates of anxiety and depressive symptoms that frequently go untreated as youth with disabilities receive treatment and support at lower rates, again likely reflecting a lack of environmental supports for youth with disabilities (National Alliance of Mental Illness [NAMI], 2022; Witt et al., 2003).
When examining gender differences in prevalence of mental health needs and supports, we also find gaps. In many epidemiological studies, women are more likely to experience internalizing mental health conditions (i.e., depression and anxiety), while men are more likely to exhibit externalizing mental health conditions (i.e., aggression, substance use; Kuehner, 2003; Mowlem et al., 2019), differences that may impact access to treatment and services. In terms of youth with disabilities, Oswald et al. (2016) found that among adolescents with and without autism, females with autism experienced anxiety and depression at higher rates than their neurotypical female counterparts, and at higher rates than males, regardless of ability status.
As caregivers and supporters through childhood, adolescence, and often into adulthood, parents are common reporters in clinical contexts during the process of diagnostic evaluation and ongoing therapy and their involvement can often be beneficial to achievement of treatment goals (Dowell & Ogle, 2010; Sun et al., 2019). Caregivers are often important conduits for supporting implementation of various change strategies (e.g., adjustments to routine, use of coping strategies, support for self-advocacy communication) identified in the psychotherapeutic process (O’Brien et al., 2013). Particularly in a health care context for adolescents, parents/ caregivers are the conduits to accessing care, as they manage the process of making and attending appointments and accessing additional supports such as medication or community resources (Logan & King, 2001). Their involvement (or not) can be the most influential factor related to help-seeking behavior in adolescents (Wahlin & Diane, 2012). Approaches parents take in the management and support of their children can have direct implications for the child or adolescent’s ability to self-regulate and to be self-directed (Steinberg, 2014). In considering self-determination, parents are often their child’s first teacher regarding opportunities to develop self-determination, and impact youth’s definition of agency, approaches to choices and decisions, and the development and implementation of environmental adaptations and accommodations (Wehmeyer, 2014). Parents/caregivers are often reporters about self-determination characteristics of adolescents, and rate skills like choice-making and decision-making as consistently important for youth with intellectual disabilities and or autism, although these skillsets are consistently rated by parents as lower than nondisabled peers (Carter et al., 2013).
While concepts of self-determination, causal agency, and self-regulated/agentic actions, and the cultivation of these characteristics have begun to make their way into community psychology and disability research literature, little is understood about the potential for integration of self-determination into psychotherapy practice (Jochems et al., 2017), or further, for the role of caregivers in supporting the development of adolescents’ self-determination as a strategy to prevent or address mental health challenges. There is a need for understanding the interplay between and among constructs associated with self-determination (volitional action, agentic action, and action-control beliefs) and behavioral-emotional regulation (internalizing symptoms, externalizing symptoms, behavioral patterns and responses, adaptive skills) to better understand the relationship between parent perceptions of self-determination and mental health, with implications for caregivers as supporters of these important characteristics in young people’s development.
Rationale for this Study
While research has demonstrated methods to support the development of self-determination and goal-directed action in students with and without disabilities in education and community settings, there is little knowledge on the relationships among caregiver-reported self-determination and behavioral-emotional characteristics that impact mental health needs in adolescents, and particularly across gender and disability status (Shogren et al., 2018). Such knowledge could further inform interventions across contexts, including caregivers in the psychotherapeutic context for adolescents with autism and/or intellectual disability.
Purpose of Study
This study sought to examine the relationships between measures of parent-reported self-determination and mental health symptomatology to examine potential relationships among these characteristics from the caregiver perspectives to inform roles for caregivers in supporting the development of self-determination and mitigation of mental health challenges. While we know that taking steps to cultivate self-determination are important for individuals to thrive, less is known about how caregivers perceive the relationship between self-determination and specific types of symptomatology adolescents may be experiencing, including problems with behavioral-emotional regulation.
Research Questions
- To what extent does disability status influence the relationship between caregiver scores on an assessment of self-determination (i.e., the Self-Determination Inventory: Parent Report) and of mental health symptomatology (i.e., internalizing and externalizing behaviors, behavioral symptoms, adaptive skills measured by the Behavior Assessment System for Children, 3rd Edition – Parent Report)?
- To what extent does gender influence the relationship between caregiver scores of an assessment of self-determination (i.e., the Self-Determination Inventory: PR) and mental health symptomatology (i.e., internalizing and externalizing behaviors, behavioral symptoms, adaptive skills measured by the Behavior Assessment System for Children, 3rd Edition – Parent Report)?
Methods
Sample and Setting
The Institutional Review Board at an academic medical center in the Midwest approved the research study. Participants were recruited from two outpatient psychotherapeutic clinics. The sample consisted of 17 participants, who self-reported demographic information. On a binary question of gender (i.e., male/female); 52.9% (N = 9) identified as male, and 47.1% (N = 8) as female. Additionally, 52.9% (N = 9) identified as nondisabled and 47.1% (N = 8) as disabled (see Table 1). For those who identified as disabled, participants were not asked to elaborate on what disabilities they experienced. Most of the sample was White/European American.
| Sex | ||||||
|---|---|---|---|---|---|---|
| Overall | Female | Male | ||||
| Demographics | n | % | n | % | n | % |
| Race | ||||||
| Two or more races | 2 | 11.8 | 0 | 0 | 2 | 22.2 |
| White/European American | 14 | 82.4 | 7 | 87.5 | 7 | 77.8 |
| Unknown | 1 | 5.9 | 1 | 12.5 | 0 | 0 |
| Ethnicity | ||||||
| Hispanic | 3 | 17.6 | 1 | 12.5 | 2 | 22.2 |
| Non-Hispanic | 14 | 82.4 | 7 | 87.5 | 7 | 77.8 |
| Age (in years) | ||||||
| 13 | 4 | 23.5 | 1 | 12.5 | 3 | 33.3 |
| 14 | 2 | 11.8 | 1 | 12.5 | 1 | 11.1 |
| 15 | 6 | 35.3 | 2 | 25.0 | 4 | 44.4 |
| 16 | 4 | 23.5 | 3 | 37.5 | 1 | 11.1 |
| Unknown | 1 | 5.9 | 1 | 12.5 | 0 | 0 |
| Therapy (in months) | ||||||
| 0 | 11 | 64.7 | 6 | 75.0 | 5 | 55.6 |
| 6 | 1 | 5.9 | 1 | 12.5 | 0 | 0 |
| 9 | 1 | 5.9 | 1 | 12.5 | 0 | 0 |
| 12 | 1 | 5.9 | 0 | 0 | 1 | 11.1 |
| 24 | 1 | 5.9 | 0 | 0 | 1 | 11.1 |
| 36 | 1 | 5.9 | 0 | 0 | 1 | 11.1 |
| 48 | 1 | 5.9 | 0 | 0 | 1 | 11.1 |
Procedures
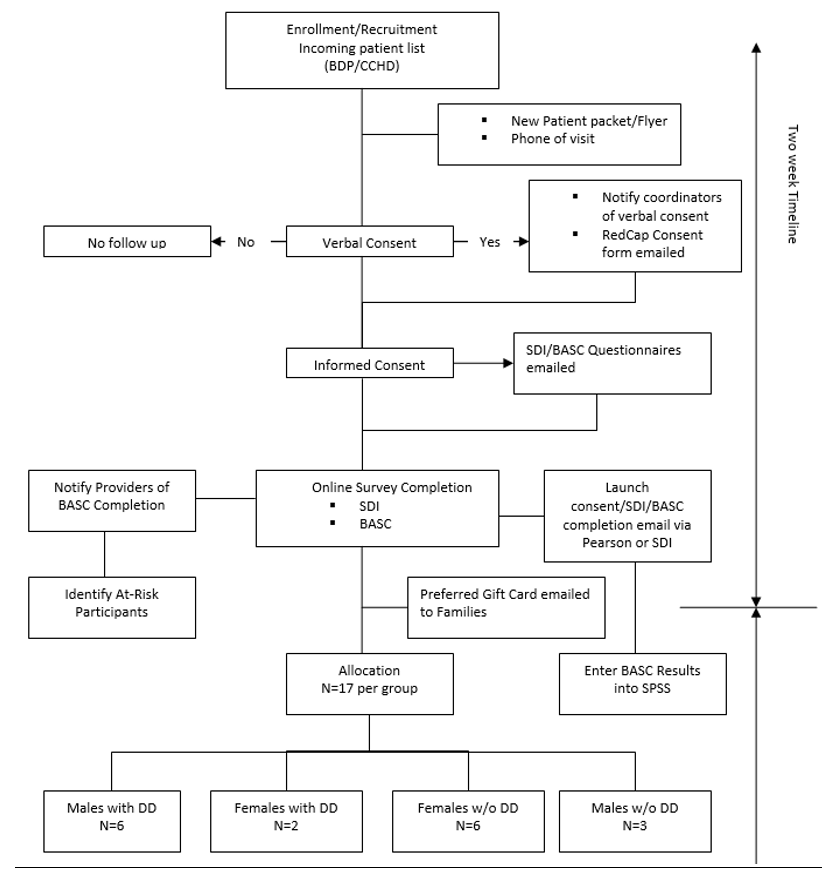
Eligibility was determined by a research team member reviewing upcoming appointments scheduled within the Developmental-Behavioral Sciences Division of the Pediatrics Department based on specific criteria (see Figure 1). To be eligible, participants needed to be between the ages of 13 and 21, English speaking, and their appointment must be an initial intake session, or they must currently be engaged in psychotherapy. Once eligibility was determined, caregivers of potential participants were called via phone and the study was explained to them. If they were interested, they were sent the consent forms via email. If BASC-3 behavior rating scales were already planned to be collected as part of their upcoming visit, we obtained permission to access those ratings in the electronic medical record. Otherwise, for all participants under 18, their caregivers were sent an email that contained a link to both the parent- and self-report BASC-3 surveys and the username and password for the self- and parent-report Self-Determination Inventory (SDI) surveys. For both the BASC-3 and SDI, there are two surveys: one for the caregiver and one for the participant. Once the youth and parent completed the two surveys, they were screened for concerning behaviors (e.g., suicidality or threats towards others). Only the parent-report data were used in the present study. If any critical items were substantially elevated, either their therapist was notified, or the participant was called directly to screen for any safety risks by the first author, a licensed psychologist. Electronic gift cards were provided to all participants upon completing study measures.
Flowchart of recruitment procedures
Measures
After consent (by either caregiver or those over 18) and assent forms (signed by participants under 18) were signed, participants or their caregivers were then linked to a demographic survey that asked about the youth participant’s age, race/ethnicity, months they had attended therapy, and gender (male/female). Once the demographics form was filled out, they were sent links to the youth and parent report versions of the two surveys: the Behavior Assessment System for Children, 3rd Edition (BASC-3) and the Self-Determination Inventory (SDI). The BASC-3 (Reynolds & Kamphaus, 2015) is a highly reliable, repeatedly validated, and commonly used measure of an individual’s expression of both adaptive as well as more challenging behaviors and thoughts, with the intent to inform intervention and ongoing monitoring. The BASC-3 Self-Report of Personality (SRP-A) version was used for adolescents aged 13-21 and the BASC-3 Parent Rating Scales for adolescents of the same age range (PRS-A) were used to collect information from parents (Reynolds & Kamphaus, 2015).The self-report forms consists of True/False and Likert type (scale 1-4, “never” to “almost always”) ratings of statements the individual may make about themselves. For parents, Likert-type ratings on the frequency with which various statements describe the teen who is the subject of the scale (scale 1-4, “never” to “almost always”) are made. This study utilized the BASC-3-PRS-A’s composite domains for analysis: externalizing problems, internalizing problems, behavioral symptoms, and adaptive skills. Table 2 shows the subdomains that correlate with their composite domain.
| Composite domain | Subdomains |
|---|---|
| Externalizing problems | Hyperactivity, aggression, conduct problems |
| Internalizing problems | Anxiety, depression, somatization |
| Behavioral symptoms | Atypicality, withdrawal, attention problems |
| Adaptive skills | Adaptability, social skills, leadership, activities for daily living, functional communication |
In addition to the BASC-3 SRP-A and PRS-A, the participants and participants’ parents were asked to complete the SDI. The SDI is a robust measurement tool that was designed to better understand self-determination in individuals and inform intervention to promote the development of causal agency. Items on the SDI have been shown to have reliability and scores to have validity in youth with and without disabilities (Shogren et al., 2017). The SDI: Student Report (SDI:SR) is completed by individuals aged 13-22 and reflects their self-perceptions of their self-determination abilities, while the SDI: Parent Report (SDI:PR) asks family members to provide reporting on their perceptions of their child’s self-determination abilities. Overall, we collected SDI:SR (N = 12), SDI:PR (N = 15), and BASC-3 PRS-A (N=17).
Bayesian Model Averaging Analysis
Supplemental materials, including scripts and data, needed to reproduce these analyses are accessible by contacting the first author, or can be found on Open Science Foundation (https://osf.io/p59ba/?view_only=26132c110c924 7388b86fcb7883ef50c). Given the sample size and the exploratory nature of our research question, we focused on exploring preliminary patterns emerging from these initial data between scores on the targeted measures in alignment with our research questions to guide future research. We used Bayesian approaches given the small sample size to evaluate the predictive power of different models examining the relationships between self-determination and BASC domains and the role of disability and gender in these relationships. Specifically, we used Bayesian Model Averaging (BMA). The logic of BMA analysis differs from null hypothesis significance testing (NHST). Traditionally, NHST aims to reject the null (M_0) in one zero/sum decision, which is difficult with reduced sample sizes that lead to low statistical power. In contrast, BMA analysis compares the probability of different models, without aiming to reject or accept them. Instead, the focus is on assessing the probabilities to determine the best model and inform ongoing research. A benefit of BMA analysis is that it leads to model comparisons that are valid with any sample size and even imprecise inferences based on small sample sizes can be continuously sharpened in later studies with larger sample sizes as evidence accumulates, which obviates the assumed need in NHST to make a zero/sum decision based on the first study ever performed (Howson & Urbach, 2006).
Bayesian Model Averaging Analysis Steps
This study implemented BMA analysis in three steps. First, the same set of general linear models was fit to data with the four BASC-3 domains (externalizing, internalizing, behavior symptoms, and adaptive skills) as the outcome variable allowing for examination of the impact of other variables of interest on the four BASC-3 domains: null (M_0); self-determination only (M_1); gender only (M_2); disability status only(M_3); self-determination moderating gender differences (M_4); and self-determination moderating disability status differences (M_5). The same set of models was repeated for both youth and parent report. Standard distribution assumptions were made for residuals. All models were estimated with ordinary least squares (OLS) using a regression procedure in the SAS 9.4 environment (PROC REG; SAS 2018). There was no missing data. It was not possible to examine a three-way interaction (self-determination, gender, and disability) because crossing gender with disability status created data sparsity in cell counts (n < 3).
Second, the fit of different models was evaluated using Bayesian Information Criterion (BIC; Ando, 2007). In BIC analysis, model fit is quantified with the BIC value (smaller is better), which balances the twin virtues of model simplicity and explanatory power. Third, BIC values were translated into model weights (McElreath, 2020). A model weight is the probability it holds the most explanatory power in the set considered. Because this study had two indices of student self-determination (self-reported vs. parent reported), a sensitivity analysis was also performed to evaluate how results of BMA analyses differ in response to relying on different types of informants of self-determination. Overall, these models allow determinations to be made about which variables, when included in the models, have the greatest probabilities of predicting BASC domain scores.
Bayesian Inferences
To address our first question (To what extent does disability status influence the relationships between caregiver scores on an assessment of self-determination and of mental health symptomatology?) and our second question (To what extent does gender influence the relationship between caregiver scores of an assessment of self-determination and mental health symptomatology?), we examined the extent to which sample data increased the probability of M_4 and M_5, respectively. Giving equal priors of 16% (=1/6) to all models in one domain, posterior model weights generated by BMA analysis close to 16% are interpreted as indicating that data really do not revise the overall probability of the model; weights under 16% indicate data reduced its probability; and weights above 16% indicate data increased its probability. As an example, a 32% weight indicates that sample data doubled the probability that this model has the most explanatory power. We further used ΔR^2 as our effect size metric (in this case, the ΔR^2 reflected the difference in R^2 between M_2 vs. M_4 to quantify the boost in explanatory power gained by adding self-determination as a moderator of gender differences and ΔR^2 reflected the difference in R^2 between M_3 vs. M_4 to quantify the boost in explanatory power gained by adding self-determination as a moderator of disability status differences). Traditionally, Cohen (1988) proposed that the borders of ”small,” “medium,” and “large” for R^2 values were 0.02, 0.13, and 0.24, respectively.
Results
Table 3 presents the main output results of BMA analysis for all outcome measures, with detailed output tables, including the regression coefficient estimates across models, for each outcome measure located in supplemental materials. Main results are that BMA analysis consistently finds across the four domains that it is highly improbable that the most explanatory model includes only self-determination (M_1), instead, these analyses suggest that it is plausible that self-determination is a moderator of predictive factors (in this case, gender and disability status; M_4 and M-5).
| Self-Determination by Disability Status (M5) | Self-Determination by Gender (M4) | |||
|---|---|---|---|---|
| SDI:PR (N=15) | SDI:PR (N=15) | |||
| BASC-3-PRS-A domains | Weight | ΔR2 | Weight | ΔR2 |
| Externalizing problems | 0.142 | 0.347 | 0.348 | 0.113 |
| Internalizing problems | 0.227 | 0.156 | 0.092 | 0.096 |
| Behavioral symptoms | 0.207 | .0433 | 0.571 | 0.317 |
| Adaptive skills | 0.414 | 0.467 | 0.443 | 0.317 |
In the sections that follow, we will review findings in alignment with our research questions as highlighted above. First, we describe the relationships among disability status and each of four BASC3 parent-report domains, when parent-reported self-determination status is included as a moderator. Next, we describe explanatory relationships among gender and each of four BASC3 parent-report domains, including self-determination status as a moderator. For each question, we describe these relationships based on parent-reported self-determination ratings.
Probability Self-Determination Moderates Disability Status Differences
In terms of the explanatory power of self-determination on the relationship between disability status and mental health characteristics (BASC3 domains), results are mixed. Findings for the explanatory patterns of self-determination as a moderator between disability status and Adaptive Skills indicated the most robust explanatory relationship for parent-reported self-determination. Parent-reported self-determination has moderate explanatory power for the relationship between disability status and Behavioral Symptoms. Model weights were also favorable for explanatory power of self-determination on the relationship between disability status and the Internalizing Symptoms domain. When examining the relationship between disability status and Externalizing Problems, the explanatory power of parent-reported self-determination as a moderator of this relationship was below the threshold of viability.
Probability Parent-Reported Self-Determination Moderates Gender Differences
Parent-reported self-determination had moderate model weights in terms of the relationship between gender and Externalizing Problems. Parent-reported self-determination had strong explanatory power for the relationship between gender and the Adaptive Skills domain. Self-determination had moderate to strong explanatory power for its impact on the relationship between gender and behavioral symptoms. In terms of self-determination’s impact on the relationship between gender status and Internalizing Symptoms, little predictive power was found. As previously noted, one should be mindful not to overinterpret the exact ∆R^2 values as we expect them to randomly fluctuate across samples of these sizes. However, they are still useful as a guide for ongoing research so long as they are not taken too literally.
Discussion
Currently little is known about how parents perceive the relationships between self-determination, gender, and disability status and mental health symptom expression. In this study, we explored how self-determination can affect the relationships between disability, gender, and mental health symptoms within a clinical sample, from a parent perspective. Understanding this interplay could better inform broader research as well as the role of parents/ caregivers in understanding or developing therapeutic targets and their role in implementing support strategies, ultimately (hopefully) improving mental health outcomes for people of all abilities. While this work is exploratory, we aimed to connect the theoretical models of mental health as well as self-determination to connect these bodies of work to support the development of these strengths-based characteristics.
Preliminary Interpretations
In this section, we will discuss implications from the BMA analysis. First, we will discuss self-determination as a moderator for the relationship between disability status (disabled or not) and mental health characteristics from the parent perspectives. Then we discuss the implications of self-determination as a moderator for the relationship between gender (male, female) and mental health characteristics.
At the outset, it is important to consider that this analysis is focused on parent report of their child’s self-determination and mental health symptomatology. However, research has shown there is not always alignment of parent and youth perspectives on youth’s self-determination (Shogren, Anderson et al., 2021) and the importance of hearing the voice of youth, particularly youth with disabilities about their self-determination and health (Shogren, Bonardi et al., 2021). Thus, future research must also explore youth’s perspectives, and how this aligns or does not align with their parents.
However, finding from the parent perspectives suggests they perceive a relatively robust relationship between overall self-determination characteristics and adaptive skills. To what extent is this finding because self-determination, as a strengths-based construct, could also be more correlated with strengths-related behaviors, such as those within the adaptive skills composite (e.g., having the skills to navigate one’s community, social contexts, and household responsibilities) needs further research. Adaptive skills have been previously recognized in the literature as predictive of self-determination for high school students with autism or intellectual disability (Tomaszewski et al., 2020). Our findings further support the hypothesis that self-determination is an important factor in psychological well-being. Further, parent’s connections between their ratings of self-determination and mental health suggests the important role of consider the family context and ways to identify potential factors to address in supporting and considering opportunities for building self-determination and adaptive skills within home contexts, particularly how these can also be aligned with efforts in mental health, community, and educational contexts.
In considering self-determination as a moderator of the relationship between disability status and various mental health characteristics, from the parent perspectives, moderate relationships were found among Self-Determination and the Internalizing and Externalizing Domains. Given that Anxiety is a subdomain of the Internalizing composite, this suggests the possibility of different pathways of relationship among depressive vs. anxious symptoms and self-determination characteristics. To better understand the relationship between self-determination characteristics and internalizing symptoms, further analysis of those internalizing symptoms from a self-report standpoint is warranted. There were also relationships between the more external behavioral scales (e.g., externalizing, behavioral symptoms) that could be more apparent to observers such as parent reporters.
Across domains, one of the most robust findings indicated that parent-reported self-determination moderates the relationship between both gender and disability status and Adaptive Skills. The Adaptive Skills scale on the BASC3 PRSA can be considered a measurement of behavioral strengths (Reynolds & Kamphaus, 2015, p. 51), measuring characteristics such as adaptability to changes, effective communication, skills associated with goal attainment, interacting with others, and organizational habits such as managing demands and other tasks. This finding begs further exploration of the relationship between self-determination and other adaptive, self-regulatory processes, such as inhibitory control and cognitive flexibility (Shogren, Mosconi et al., 2021) and the implications these processes have on such factors as emotional regulation and corresponding mental health symptomatology. Caregiver perspectives are integral to this continued exploration as
Causal Agency Theory recognizes the interdependence of goal setting for all people and the role of context in shaping the expression of self-determination abilities. A self-determined person has agency over their goal-directed actions, even if that means empowering others to make or implement decisions based on the values, preferences, and beliefs communicated by the person. (Shogren, Mosconi et al., 2021, p. 291)
Understanding the perspectives of these interdependent support people, such as caregivers and parents, can further inform support design.
Another interesting finding was that the least predictive power for the model in which self-determination moderates gender differences is internalizing symptoms. This could be, in part, because parent reporters can only presuppose the internal processes of the adolescents about whom they are reporting, by reporting about observable behavioral characteristics. Given the least predictive power found for this relationship, it could suggest that self-determination may not be as much of a moderator of the relationship between gender and internalizing symptoms from parent perspectives. However, more data is needed to further evaluate this hypothesis. In the case of this study’s data, we had a very low number of females with disabilities, which could have contributed to the results found here. A moderate explanatory relationship was indicated for the predictive power of Self-Determination and the Behavioral Symptoms composite as well as for Self-Determination and Externalizing composite when gender was included in the model. Interestingly, this suggests that there may be more of an explanatory relationship for self-determination’s impact on externalizing vs. internalizing symptoms, across both gender and disability status. If so, the therapeutic implications could include a closer focus on development of skills related to self-determination, particularly related to self-awareness, self-monitoring, and other self-regulation strategies. Certainly, there should be a focus in future work on better understanding the relationship between self-report self-determination characteristics and self-report of more internalizing symptoms such as anxiety or depression, to further evaluate this potential relationship. There may be further to examine in terms of the role of self-regulation as relates to both self-determination and externalizing behavior characteristics.
When examining the explanatory relationship of self-determination on the relationship between externalizing behaviors and gender or disability status, moderate explanatory relationships were found. This raises additional interesting questions about the nature of self-determination’s potential role or relationship to such self-regulatory factors as inhibition, and potential pathways of influence among self-determination and externalizing behaviors and other mental health characteristics. For example, further analysis of specific executive processes, such as inhibitory control, or cognitive flexibility could be helpful in better understanding the role of these executive processes in self-determination as well as emotion regulation (Shogren, Mosconi, et al., 2021). In addition, the “hotter” executive processes could also be of interest given their role in affect and emotional expression and self-regulation, particularly for autistic individuals (Demetriou et al., 2019). Considering the various constructs contributing to self-determination, there is also more to explore in terms of specific components, such as action-control beliefs and their relationship to executive function constructs related to self-regulation (Vanlede et al., 2006). There is no doubt a need for additional research to explore the relationship among these characteristics to understand their impact for individuals with and without disabilities.
From a supports standpoint, better understanding of these relationships could inform adaptations to psychotherapeutic approaches as well as incorporation of particular parenting strategies to promote self-determination and social emotional health. For example, if it is found that self-determination and more externalizing symptoms are connected and mutually influence one another, guidance for parents and support for teens in promoting opportunities to practice self-monitoring, self-evaluation, and self-management could be of particular importance within the development of a psychotherapy support plan. Similarly, if the interconnection of adaptive skills and self-determination holds, specific strategies could be implemented to increase teens’ opportunities to engage in problem solving, particularly related to navigating practical, social, and other community contexts of importance to the teen and their goals.
Limitations
Reduced sample sizes led to low power, which made traditional null hypothesis testing unfeasible. We only had parent reported data (SDI:PR) from 15 participants. This study was conceptualized before the pandemic but implemented during the pandemic, making it necessary to be conducted in a telehealth environment. This may account for the small sample size. To compensate, we fit a series of models to data of varying complexity and relied on BMA analysis techniques to compare the probability of one of these different models to see which is the most explanatory, without necessarily rejecting or accepting them. This provides key direction for future research, but these results must be considered exploratory.
We hypothesized that a three-order interaction between self-determination, gender, and disability status may increase explanatory power. However, we were not able to include a model with a three-way interaction because crossing gender with disability status created small cell counts. However, this study did find promising evidence in at least some domains that tentatively suggests that self-determination could moderate both gender differences and moderate disability status relationship to mental health symptoms, which opens the door in future studies to investigate three-way interactions between these factors.
In addition, because of the small sample size, analyses of BASC-3 data focused on the composite domains (Internalizing, Externalizing, Behavioral Symptoms, and Adaptive Skills) and subdomains were not evaluated. Similarly, analysis of the SDI data focused on the overall self-determination score, rather than subdomains. Future research could incorporate analysis at the subdomain level to examine potential pathways of relationship more closely between subdomains, such as that between Action-Control Beliefs and Internalizing Symptoms such as anxiety or depression.
Finally, this study focused only on parent-reported data. This provides an analysis focused on the perspectives of caregivers on their teens’ context. While this is valuable information, especially considering the key support role parents and caregivers play in identifying, accessing, and supporting mental health needs and their potential role in the development of self-determination of adolescents, it is important to be clear that parent perspective does not capture the young person’s experience. Future work should incorporate and synthesize findings from individual as well as parent/caregiver perspective. Work could also incorporate additional contextual variables such as social supports, school connectedness, or measures of other internal characteristics such as internalized ablism, or degree of parent/caregiver internalizing or externalizing symptoms.
Conclusions
In this study, we explored patterns of relationships between self-determination and mental health symptomatology within a clinically referred sample of adolescents with and without disabilities. While sample size is limited, results of Bayesian analysis suggest that there are potential relationships among these variables that warrant further exploration, warranting ongoing work. More research is needed to better elucidate these relationships and their impact for research and mental health practice.
References
Ando, T. (2007). Bayesian predictive information criterion for the evaluation of hierarchical Bayesian and empirical Bayes models. Biometrika, 94(2), 443-458. https://doi.org/10.1093/biomet/asm017
Carter, E. W., Lane, K. L., Cooney, M., Weir, K., Moss, C. K., & Machalicek, W. (2013). Parent assessments of self-determination importance and performance for students with autism or intellectual disability. American Journal on Intellectual and Developmental Disabilities, 118(1), 16-31. https://doi.org/10.1352/1944-7558-118.1.16
Deci, E. L., & Ryan, R. M. (2012). Self-determination theory. In P. A. M. Van Lange, A. W. Kruglanski, & E. T. Higgins (Eds.), Handbook of theories of social psychology (pp. 416–436). Sage Publications Ltd. https://doi.org/10.4135/9781446249215.n21
DeFilippis, M. (2018). Depression in children and adolescents with autism spectrum disorder. Children, 5(9). https://doi.org/10.3390/children5090112
Demetriou, E. A., DeMayo, M. M., & Guastella, A. J. (2019). Executive function in autism spectrum disorder: History, theoretical models, empirical findings, and potential as an endophenotype. Frontiers in Psychiatry, 10. https://doi.org/10.3389/fpsyt.2019.00753
Diamond, L. M., & Aspinwall, L. G. (2003). Integrating diverse developmental perspectives on emotion regulation. Motivation and Emotion, 27, 1-6. https://doi.org/10.1023/A:1023670208060
Dowell, K. A., & Ogles, B.M. (2010). The effects of parent participation on child psychotherapy outcome: A meta-analytic review. Journal of Clinical Child and Adolescent Psychology, 39(2), 151-162. https://doi.org/10.1080/15374410903532585
Howson, C., & Urbach, P. (2006). Scientific reasoning: The Bayesian approach. Open Court Publishing.
Jochems, E. C., Duivenvoorden, H. J., van Dam, A., van der Feltz‐Cornelis, C. M., & Mulder, C. L. (2017). Motivation, treatment engagement and psychosocial outcomes in outpatients with severe mental illness: A test of self‐determination theory. International Journal of Methods in Psychiatric Research, 26(3). https://doi.org/10.1002/mpr.1537
Kuehner, C. (2003). Gender differences in unipolar depression: an update of epidemiological findings and possible explanations. Acta Psychiatrica Scandinavica, 108(3), 163-174. https://doi.org/10.1034/ j.1600-0447.2003.00204.x
Lauer, E. A., & Lauer, E. (2019). Assessing the association between mental health and disability indicators among adults living in the United States. Disability and Health Journal, 12(1), 98-105. https://doi.org/10.1016/j.dhjo.2018.08.006
Little, T. D., Snyder, C. R., & Wehmeyer, M. (2006). The agentic self: On the nature and origins of personal agency across the lifespan. In D. Mroczek & T. D. Little (Eds.), Handbook of personality development (pp. 61–80). LEA.
Logan, D. E., & King, C. A. (2001). Parental facilitation of adolescent mental health service utilization: A conceptual and empirical review. Clinical Psychology: Science and Practice, 8(3), 319-333. https://psycnet.apa.org/doi/10.1093/clipsy.8.3.319
McElreath, R. (2020) Statistical rethinking: A Bayesian course with examples in R and STAN (2nd ed.). CRC Press.
Mowlem, F., Agnew-Blais, J., Taylor, E., & Asherson, P. (2019). Do different factors influence whether girls versus boys meet ADHD diagnostic criteria? Sex differences among children with high ADHD symptoms. Psychiatry Research, 272, 765-773. https://doi.org/10.1016/j.psychres.2018.12.128
National Alliance of Mental Illness. (2022.). People with disabilities. https://www.nami.org/Your-Journey/Identity-and-Cultural-Dimensions/People-with-Disabilities
O’Brien, M., Crickard, E., Lee, J., & Holmes C. (2013). Attitudes and experience of youth and their parents with psychiatric medication and relationship to self-reported adherence. Community Mental Health Journal, 49, 567–575. https://doi.org/10.1007/s10597-012-9526-x
Oswald, T. M., Winter-Messiers, M. A., Gibson, B., Schmidt, A. M., Herr, C. M., & Solomon, M. (2016. Sex differences in internalizing problems during adolescence in autism spectrum disorder. Journal of Autism and Developmental Disorders, 46(2), 624–636. https://doi.org/10.1007/s10803-015-2608-1
Reynolds, C. R., & Kamphaus, R. W. (2015). Behavior assessment for children (BASC-3, 3rd ed.). [Assessment Instrument]. Pearson.
Shogren, K. A., Anderson, M. H., Raley, S. K., & Hagiwara, M. (2021). Exploring the relationship between student & teacher/proxy-respondent scores on the Self-Determination Inventory. Exceptionality, 29(1), 47-60. https://doi.org/10.1080/09362835.2020.1729764
Shogren, K. A., Bonardi, A., Cobranchi, C., Krahn, G., Murray, A., Robinson, A., Havercamp, S. M., & The Nisonger RRTC on Health and Function. (2021). State of the Field: The need for self-report measures of health and quality of life for people with intellectual and developmental disabilities. Journal of Policy and Practice in Intellectual Disabilities, 18(4), 286-295. https://doi. org/10.1111/jppi.12386
Shogren, K. A., Burke, K. M., Anderson, M. H., Antosh, A. A., Wehmeyer, M. L., LaPlante, T., & Shaw, L. A. (2018). Evaluating the differential impact of interventions to promote self-determination and goal attainment for transition-age youth with intellectual disability. Research and Practice for Persons with Severe Disabilities, 43(3), 165-180. https://doi.org/10.1177/1540796918779775
Shogren, K. A., Gross, J. M., Forber-Pratt, A. J., Francis, G. L., Satter, A. L., Blue-Banning, M., & Hill, C. (2015). The perspectives of students with and without disabilities on inclusive schools. Research and Practice for Persons with Severe Disabilities, 40(4), 243–260. https://doi.org/10.1177/ 1540796915583493
Shogren, K. A., Lopez, S. J., Wehmeyer, M. L., Little, T. D., & Pressgrove, C. L. (2006). The role of positive psychology constructs in predicting life satisfaction in adolescents with and without cognitive disabilities: An exploratory study. The Journal of Positive Psychology, 1(1), 37–52. https://doi.org/ 10.1080/17439760500373174
Shogren, K. A., Mosconi, M. W., Raley, S. K., Dean, E. E., Edwards, B., Wallisch, A. Boyd, B., & Kiblen, J. C. (2021). Advancing the personalization of assessment and intervention in autistic adolescents and young adults by targeting self-determination and executive processes. Autism in Adulthood, 3(4), 289-299. https://doi.org/10.1089/aut.2021.0010
Shogren, K. A., & Raley, S. K. (2022). Self-determination and causal agency theory: Integrating Research into Practice. Springer.
Shogren, K. A., Wehmeyer, M. L., Little, T. D., Forber-Pratt, A. J., Palmer, S. B., & Seo, H. (2017). Preliminary validity and reliability of scores on the Self-Determination Inventory: Student Report version. Career Development and Transition for Exceptional Individuals, 40(2), 92-103. https://doi.org/ 10.1177/2165143415594335
Steinberg, L. (2014). Age of opportunity: Lessons from the new science of adolescence. Houghton Mifflin Harcourt.
Sun, M., Rith-Najarian, L. R., Williamson, T. J., & Chorpita, B. F. (2019) Treatment features associated with youth cognitive behavioral therapy follow-up effects for internalizing disorders: A meta-analysis. Journal of Clinical Child Adolescent Psychology. https://doi.org/10.1080/15374416.2018. 1443459
Tomaszewski, B., Kraemer, B., Steinbrenner, J. R., Smith DaWalt, L., Hall, L. J., Hume, K., & Odom, S. (2020). Student, educator, and parent perspectives of self‐determination in high school students with autism spectrum disorder. Autism Research, 13(12), 2164-2176. https://doi.org/10.1002/ aur.2337
Vanlede, M., Little, T. D., & Card, N. A. (2006) Action-control beliefs and behaviors as predictors of change in adjustment across the transition to middle school, Anxiety, Stress, & Coping, 19(2), 111-127. https://doi.org/10.1080/10615800600632896
Van Steensel, F. J., Bögels, S. M., & Perrin, S. (2011). Anxiety disorders in children and adolescents with autistic spectrum disorders: A meta-analysis. Clinical Child and Family Psychology Review, 14, 302-317. https://doi.org/10.1007/s10567-011-0097-0
Wahlin T., & Deane F. (2012). Discrepancies between parent-and adolescent-perceived problem severity and influences on help seeking from mental health services. Australian and New Zealand Journal of Psychiatry, 46, 553–560. https://doi.org/10.1177/0004867412441929
Wehmeyer, M. L. (2014). Self‐determination: A family affair. Family Relations, 63(1), 178-184. https://doi.org/10.1111/fare.12052
Witt, W. P., Kasper, J. D., & Riley, A. W. (2003). Mental health services use among school-aged children with disabilities: The role of sociodemographics, functional limitations, family burdens, and care coordination. Health Services Research, 38(6p1), 1441–1466. https://doi.org/10.1111/j.1475-6773.2003.00187.x
