Spencer Fox Eccles School of Medicine
35 Observing the Link Between Neural Activation Patterns and Motor Performance in MDD
Joy Akindulureni and Vincent Koppelmans
Faculty Mentor: Vincent Koppelmans (Psychiatry, University of Utah)
Background
Major Depressive Disorder (MDD) affects millions of people worldwide as it has been ranked the third cause of the burden of disease (Bains & Abdijadid, 2023). The severity of the condition is shown by the fact that 20% of untreated individuals with MDD will attempt suicide. With numerous treatments from medications to psychotherapy, some patients might still demonstrate resistance to these conventional approaches. This makes it critical to develop tools that could effectively improve treatment outcomes for individuals with MDD.
Previous research has shown the cognitive and emotional domains that MDD can affect, however there is still limited understanding in the effects of MDD on motor deficits (Wuthrich et al, 2024). We are investigating the neural differences in motor function between individuals with depression and control subjects. By doing a squeeze task done by participants to assess neural activation in the primary motor cortex, we can examine motor function deficits in depression and potentially classify depression subtypes. Understanding the neural differences in motor function between individuals with depression and control subjects is crucial for having a deeper understanding of depression and treatment methods.
Further examination into the motor function of structural and functional integrity using Magnetic Resonance Integrity (MRI) data. Previous investigations have revealed differences in activation between people with MDD and controls in brain regions like the motor cortex, thalamus and cerebellum which are critical for neural control of movement (Tura & Goya-Madonaldo, 2023). Like previous studies, our study implements the use of a motor task with grip strength to find activation in motor cortex and be able to understand more on motor deficits in depression, because grip strength is a pure motor measure that requires no cognitive effort and which elicits a clear signal in the primary motor cortex, we predict that depressed individuals have more motor deficits and less neural activation compared to individuals without depression. By including the motor task measure, the aim is to provide a deeper insight into the neurobiology of MDD and its role in motor dysfunction. This approach will enhance the understanding of motor abnormalities in MDD and evaluate their potential as valid biomarkers for the disorder.
Methodology
Participant recruitment
Control and depressed participants aged 18 years and older with 22 subjects being part of the control group and 18 subjects being part of the depressed group (Mean age = 30.68; Female (27); Male (13)] were recruited both in-person and online through written advertisements, referrals, and from several online databases. Prospective participants then completed a series of interviews and screenings to determine their eligibility and undergo group classification. Patients identified with MDD and trMDD were also specifically referred by a psychiatrist from the Treatment Resistant Depression clinic within the Huntsman Mental Health Institute at the University of Utah.
Interview process / Inclusion and Exclusion Criteria
Control and depressed participants aged 18 years and older with 22 subjects being part of the control group and 18 subjects being part of the depressed group (Mean age = 30.68; Female (27); Male (13)] were recruited both in-person and online through written advertisements, referrals, and from several online databases. Prospective participants then completed a series of interviews and screenings to determine their eligibility and undergo group classification. Patients identified with MDD and trMDD were also specifically referred by a psychiatrist from the Treatment Resistant Depression clinic within the Huntsman Mental Health Institute at the University of Utah.
During the scheduled meeting, the consent form was emailed to them through the REDCap survey system for them to sign electronically. The Mini International Neuropsychiatric Interview (MINI) was administered to ensure that participants with potential depression did not have any confounding psychiatric illnesses. For controls, the MINI was used to ensure that they did not present with any confounding psychiatric features: Bipolar disorder, Major Depressive Disorder, or any eating disorders. If they were determined as a control, they were scheduled for the visit and if they presented as depressed, they were scheduled to do the Hamilton Depression Scale test (HAM-D) to determine the severity of their depression.
Before the first visit, participants would be sent a link to complete several online questionnaires including: Patient Health Questionnaire (PHQ-9), Generalized Anxiety Disorder Scale (GAD-7), World Health Organization Quality of Life (WHOQOL-BREF), and the Dutch handedness questionnaire. The completion time for control subjects with the procedures is 60 minutes and 100 minutes (about 1 and a half hours) for depressed subjects.
Visit Procedures
The 1st visit consisted of completing the MRI scan followed by motor and cognitive testing. Arrival at the MRI center included an MRI screening test that all participants completed upon arrival to reevaluate the potential for any contraindications for the MRI which would also include pregnancy for female participants. The MRI scan was conducted on a Siemens Prisma 3T research scanner. During a functional MRI scan, participants had to complete a hand squeeze task as they looked at an ellipse while it turned green and release when it turned red, intended to elicit activation in the primary motor cortex. The full scan protocol included sequences to obtain measures of brain volume, white matter structure, and brain activation as the participant squeezed their hand when the color of the target changed. Depressed participants had to complete the HAM-D again before their second visit. Participants were invited back to complete their second visit three months after their first visit to detect for any potential changes in hand squeeze performance related to changes in symptoms of depression or remission.
MRI Protocol and Data Analysis
During MRI scans, the protocol used for the MRI was intended to capture anatomical and functional data. The scan sequences implemented to record anatomical data were T1 weighted images (TE = 1ms, TR = 2.5ms, Flip Angle = 8°, FoV = 93.75mm). For our functional data (TE =1ms, TR = 0.8ms, Flip Angle = 52°, FoV = 100mm), we conducted preprocessing and first level analysis.
All data was converted using Brain Imaging Data Structure (BIDS) which takes the raw DICOM images from brain scans into bids-compliant format for processing later. BIDS allows for the use of predefined pipeline as it ensures that all data are named using a known convention with meta data (e.g., scan parameter) accompanied in the form of .json files. This helps in the sharing of data within and between labs to make sure that the dataset is organized (Gorgolewski et al., 2016). After BIDSification of data, we used fMRIprep which performs basic preprocessing steps: Coregistration, realignment, normalization to the Montreal Neurological Institute (MNI) template brain, brain extraction, segmentation, and skull stripping. It also provides a large variety of covariates (motion parameters, motion outliers, steady state outliers, white matter and CSF signal) that can be used in first level analyses later. fMRIprep is an open-source software that keeps data to a standardized level and prevents human error because of its automated computerized process. By using fMRIprep it makes it easier to use compared to other data processing software. We used Statistical Parametric Mapping 12 (SPM) software running under MATLAB. for smoothing to reduce noise at [8 8 8] full width at half maximum (FWHM). For the first level analysis, we created a contrast to see the activation at the individual level. For first level analysis, we used SPM12 and built the design matrix by using the following regressors: rotation and translation in x,y,z axis which accounts for head motion in the three spatial axes, motion outliers which help in detecting excessive movements, CompCor (Component noise correction method) detects for noise and helps to reduce the noise and steady state outliers detected at the start of the scan. The design matrix is a model which gives predictors and variables for analyzing task related fMRI scans. We focused on the hand squeeze task and th contrast was defined as the squeeze condition compared to when they were at rest (squeeze > crosshair). This helps in identifying brain regions involved in the motor task of hand squeezing. For group level analysis, Analysis of Variance (ANOVA) will be conducted to test for differences in activation in the primary motor cortex between control subjects and depressed subjects for the second level analysis.
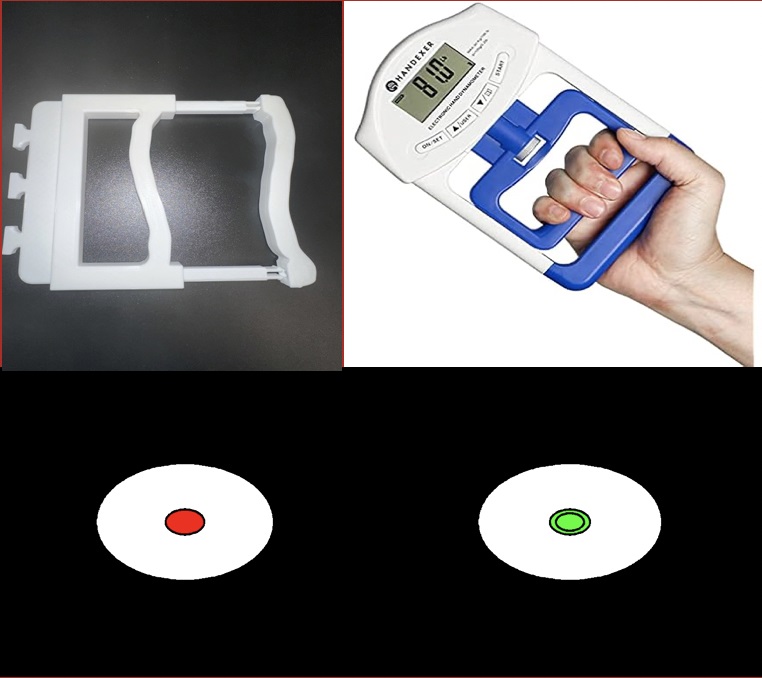
Figure 1: Squeeze task and calibration device (Up); The target ellipse when it turns from red to green (Down)
Results
Results from our first level analysis show that, at the individual level, contrasts comparing hand squeezing and rest showed strong activations in the primary motor cortex and associated areas (e.g., premotor cortex and supplementary motor area). An example of these results is shown in Figure 2. For some subjects, neural activation was also observed in the visual cortex, potentially since subjects were focusing more on the task presentation while hand squeezing than during rest periods.
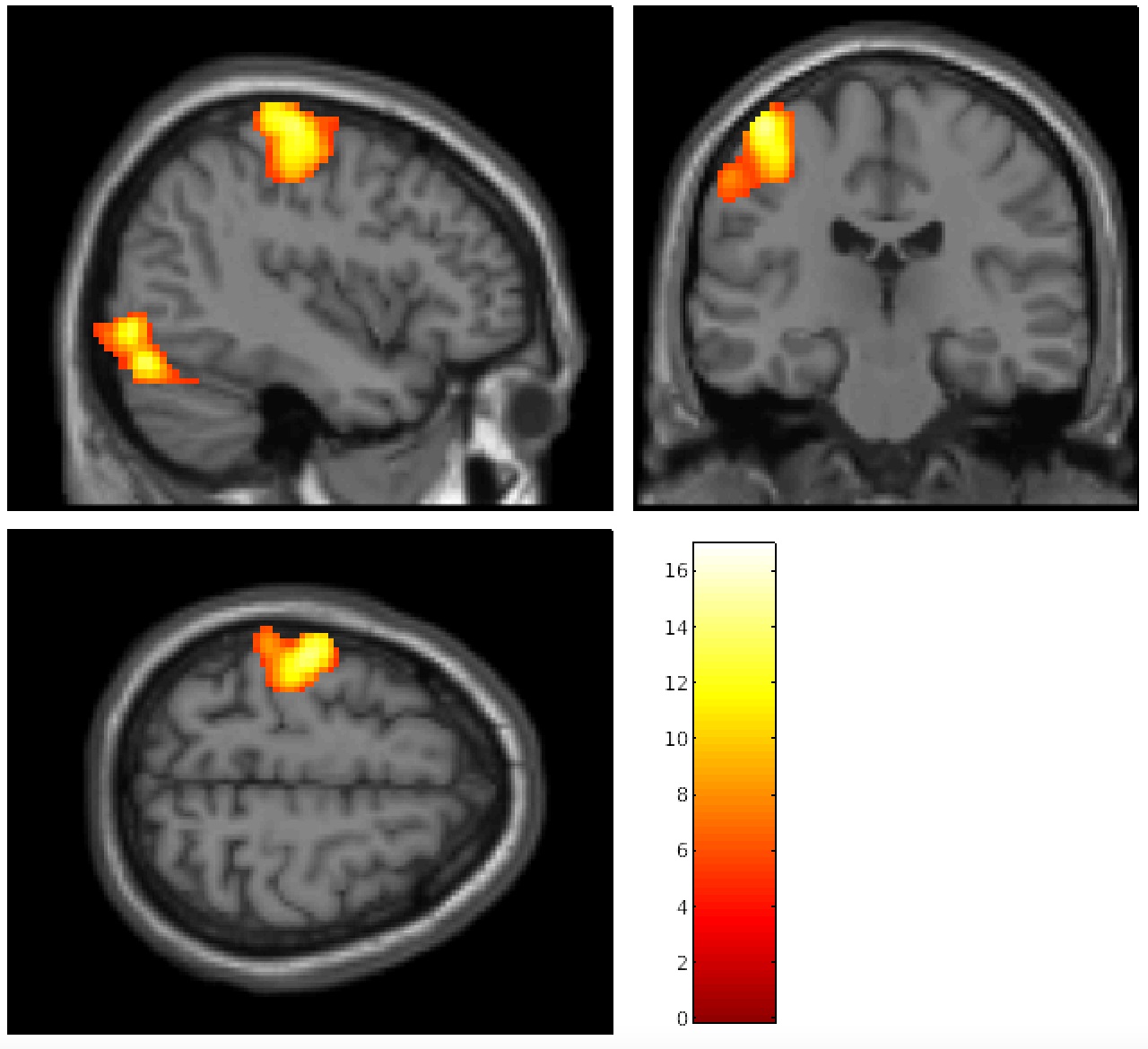 Figure 2: MNI template with activation of the primary motor cortex for squeeze compared to rest after contrast for a single subject
Figure 2: MNI template with activation of the primary motor cortex for squeeze compared to rest after contrast for a single subject
Conclusion and Future Directions
Results from our first level analyses show that we can reliably elicit brain activation in the primary motor cortex at the individual level. This is an important first step to be able to detect potential associations between neural motor function and major depression. A second level analysis will be conducted to examine this hypothesis by testing the differences between the depressed and control groups in primary motor cortex activation. We are also looking to explore the patterns of brain activity associated with cognitive and motor impairments in participants with depression compared to healthy controls. A limitation of our work is the sample size which could reduce generalizability. When sample size is small, results may not effectively represent the diversity in the population which can lead to biased results. In future work we will aim to expand our current sample to increase the robustness of our results.
Bibliography
Media Attributions
- 137489262_fig_1
- 146879582_fig_2
