Jonathan Akin
Unit Outline
- Flexion and Extension
- Hyperextension
- Abduction and Adduction
- Circumduction
- Rotation
- Supination and Pronation
- Dorsiflexion and Plantar Flexion
- Inversion and Eversion
- Protraction and Retraction
- Depression and Elevation
Learning Objectives
At the end of this unit, you should be able to:
I. Describe the levels of muscle organization: fascia, fascicles, muscle fibers.
II. Describe the following structures of a muscle cell: sarcolemma, sarcoplasm, nuclei, mitochondria, sarcoplasmic reticulum, transverse tubules, myofibrils, myofilaments, sarcomere.
III. Describe the following structures of a sarcomere: Z line, I band, A band, H zone, M line.
IV. Describe the basic structure of the thick and thin filaments and their primary protein components.
V. Specify four factors that determine the type of movement accomplished by a muscle.
VI. Specify some of the criteria used in the naming of muscles.
VII. Describe, using specific examples, 16 types of movements characteristic of skeletal muscle contractions.
Part 1: Muscle Tissue
When most people think of muscles, they think of the muscles that are visible just under the skin, particularly of the limbs. These are skeletal muscles, so named because most of them move the skeleton. But there are two other types of muscles in the body, with distinctly different jobs. Cardiac muscle, found in the heart, is concerned with pumping blood through the circulatory system. Smooth muscle is concerned with various involuntary movements, such as having one’s hair stand on end when cold or frightened, or moving food through the digestive system. This chapter will examine the structure and function of these three types of muscles.
Overview of Muscle Tissues
Muscle is one of the four primary tissue types of the body, and the body contains three types of muscle tissue: skeletal muscle, cardiac muscle, and smooth muscle (Figure 13.1). All three muscle tissues have some properties in common; they all exhibit a quality called excitability, as their plasma membranes can change their electrical states (from polarized to depolarized) and send an electrical wave called an action potential along the entire length of the membrane. While the nervous system can influence the excitability of cardiac and smooth muscle to some degree, skeletal muscle completely depends on signaling from the nervous system to work properly. On the other hand, both cardiac muscle and smooth muscle can respond to other stimuli, such as hormones and local signals.
The processes of muscle contraction (shortening) and relaxation (return to its resting length) will be explained in the next chapter. A muscle can return to its original length when relaxed due to a quality of muscle tissue called elasticity. It can recoil back to its original length due to elastic fibers. Muscle tissue also has the quality of extensibility; it can stretch or extend. Contractility allows muscle tissue to pull on its attachment points and shorten with force.
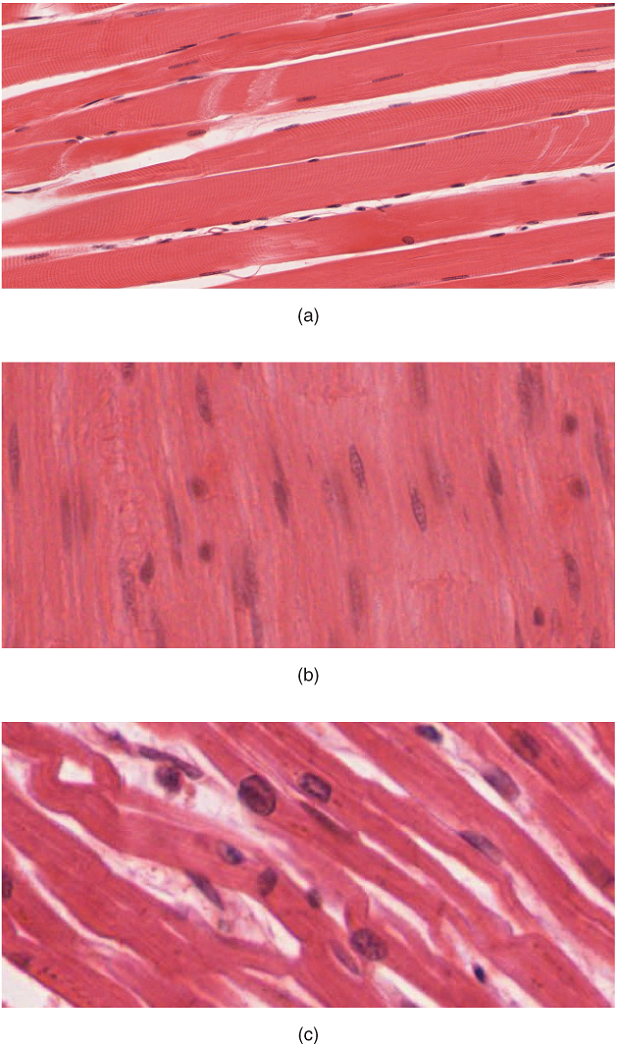
Differences among the three muscle types include the microscopic organization of their contractile proteins—actin and myosin. The actin and myosin proteins are arranged very regularly in the cytoplasm of individual muscle cells (referred to as fibers) in both skeletal muscle and cardiac muscle, which creates a pattern of stripes, called striations. The striations are visible with a light microscope under high magnification (Figure 13.1). Skeletal muscle fibers are multinucleated structures that compose the skeletal muscle. Cardiac muscle fibers each have one to two nuclei and are physically and electrically connected to each other so that the entire heart contracts as one unit (called a syncytium).
Because the actin and myosin are not arranged in such regular fashion in smooth muscle, the cytoplasm of a smooth muscle fiber (which has only a single nucleus) has a uniform, non-striated appearance (resulting in the name smooth muscle). However, the less organized appearance of smooth muscle should not be interpreted as less efficient.
Smooth muscle in the walls of arteries is a critical component that regulates blood pressure necessary to push blood through the circulatory system; and smooth muscle in the skin, visceral organs, and internal passageways is essential for moving all materials through the body.
Skeletal Muscle
The best-known feature of skeletal muscle is its ability to contract and cause movement. Skeletal muscles act not only to produce movement but also to stop movement, such as resisting gravity to maintain posture. Small, constant adjustments of the skeletal muscles are needed to hold a body upright or balanced in any position. Muscles also prevent excess movement of the bones and joints, maintaining skeletal stability and preventing skeletal structure damage or deformation. Joints can become misaligned or dislocated entirely by pulling on the associated bones; muscles work to keep joints stable. Skeletal muscles are located throughout the body at the openings of internal tracts to control the movement of various substances. These muscles allow functions, such as swallowing, urination, and defecation, to be under voluntary control. Skeletal muscles also protect internal organs (particularly abdominal and pelvic organs) by acting as a barrier or shield to external trauma and by supporting the weight of the organs.
Skeletal muscles contribute to the maintenance of homeostasis in the body by generating heat. Muscle contraction requires energy, and when ATP is broken down, heat is produced. This heat is very noticeable during exercise, when sustained muscle movement causes body temperature to rise, and in cases of extreme cold, when shivering produces random skeletal muscle contractions to generate heat.
Each skeletal muscle is an organ that consists of various integrated tissues. These tissues include the skeletal muscle fibers, blood vessels, nerve fibers, and connective tissue. Each skeletal muscle has three layers of connective tissue (called “mysia”) that enclose it and provide structure to the muscle as a whole, and also compartmentalize the muscle fibers within the muscle (Figure 13.2). Each muscle is wrapped in a sheath of dense, irregular connective tissue called the epimysium, which allows a muscle to contract and move powerfully while maintaining its structural integrity. The epimysium also separates muscle from other tissues and organs in the area, allowing the muscle to move independently.
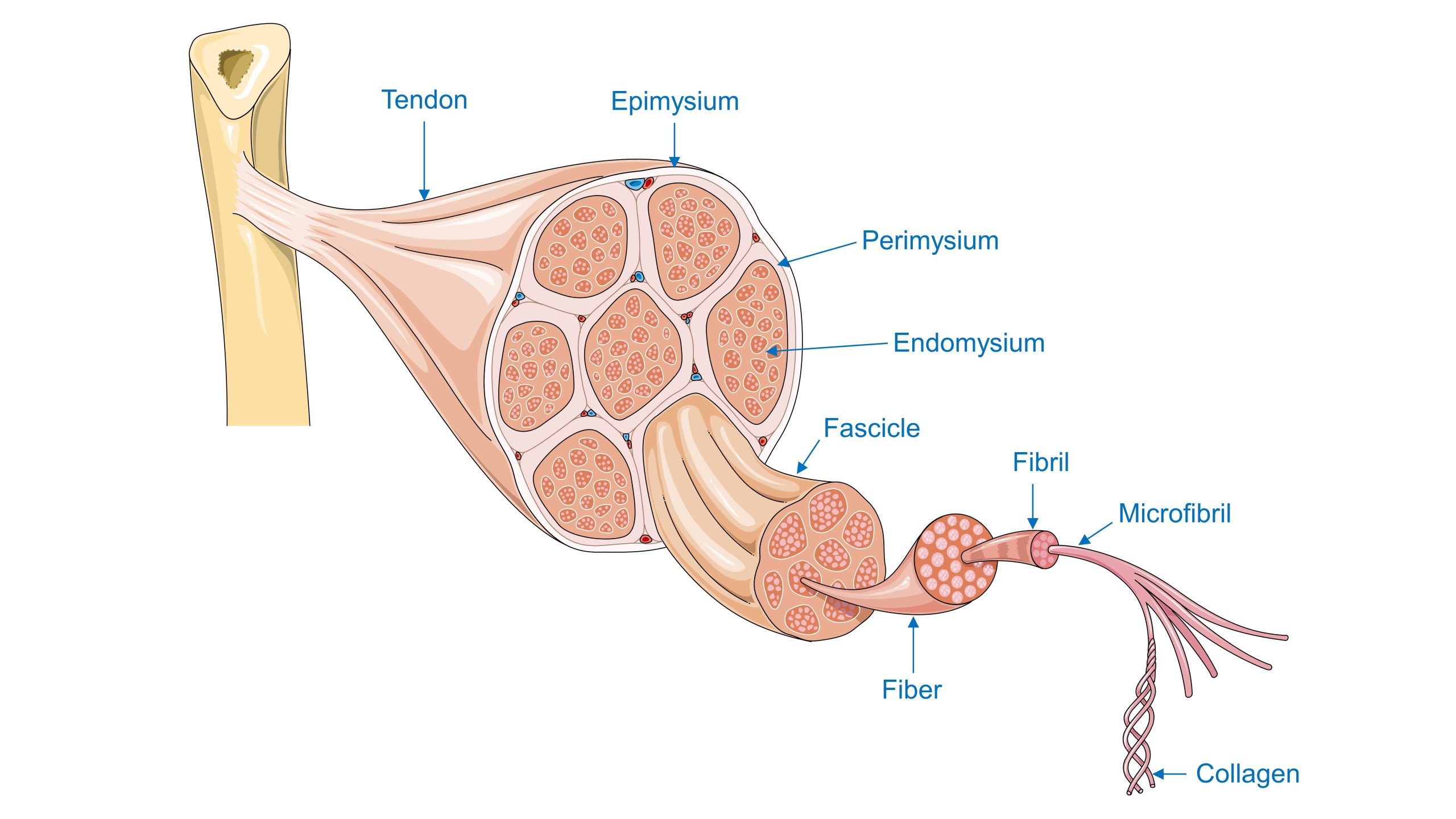
Inside each skeletal muscle, muscle fibers are organized into individual bundles, each called a fascicle, by a middle layer of connective tissue called the perimysium. This fascicular organization is common in muscles of the limbs; it allows the nervous system to trigger a specific movement of a muscle by activating a subset of muscle fibers within a bundle, or fascicle of the muscle. Inside each fascicle, each muscle fiber is encased in a thin connective tissue layer of collagen and reticular fibers called the endomysium. The endomysium contains the extracellular fluid and nutrients to support the muscle fiber. These nutrients are supplied via blood to the muscle tissue.
In skeletal muscles that work with tendons to pull on bones, the collagen in the three tissue layers (the mysia) intertwines with the collagen of a tendon. At the other end of the tendon, it fuses with the periosteum coating the bone. The tension created by the contraction of the muscle fibers is then transferred through the mysia, to the tendon, and then to the periosteum to pull on the bone for movement of the skeleton.
Every skeletal muscle is also richly supplied by blood vessels for nourishment, oxygen delivery, and waste removal. In addition, every muscle fiber in a skeletal muscle is innervated by the axon branch of a somatic motor neuron, which signals the fiber to contract. Unlike cardiac and smooth muscle, the only way to functionally contract a skeletal muscle is through signaling from the nervous system.
Skeletal Muscle Fibers
Because skeletal muscle cells are long and cylindrical, they are commonly referred to as muscle fibers. Skeletal muscle fibers can be quite large for human cells, with diameters up to 100 μm and lengths up to 30 cm (11.8 in) in the sartorius of the upper leg. During early development, embryonic myoblasts, each with its own nucleus, fuse with up to hundreds of other myoblasts to form the multinucleated skeletal muscle fibers. Multiple nuclei mean multiple copies of genes, permitting the production of the large amounts of proteins and enzymes needed for muscle contraction.
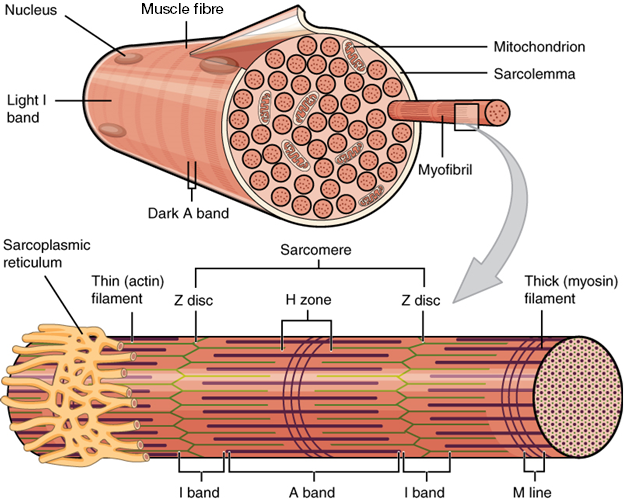
Some other terminology associated with muscle fibers is rooted in the Greek sarco, which means “flesh.” The plasma membrane of muscle fibers is called the sarcolemma, the cytoplasm is referred to as sarcoplasm, and the specialized smooth endoplasmic reticulum, which stores, releases, and retrieves calcium ions (Ca++) is called the sarcoplasmic reticulum (SR) (Figure 13.3). As will soon be described, the functional unit of a skeletal muscle fiber is the sarcomere, a highly organized arrangement of the contractile myofilaments actin (thin filament) and myosin (thick filament), along with other support proteins.
The Sarcomere
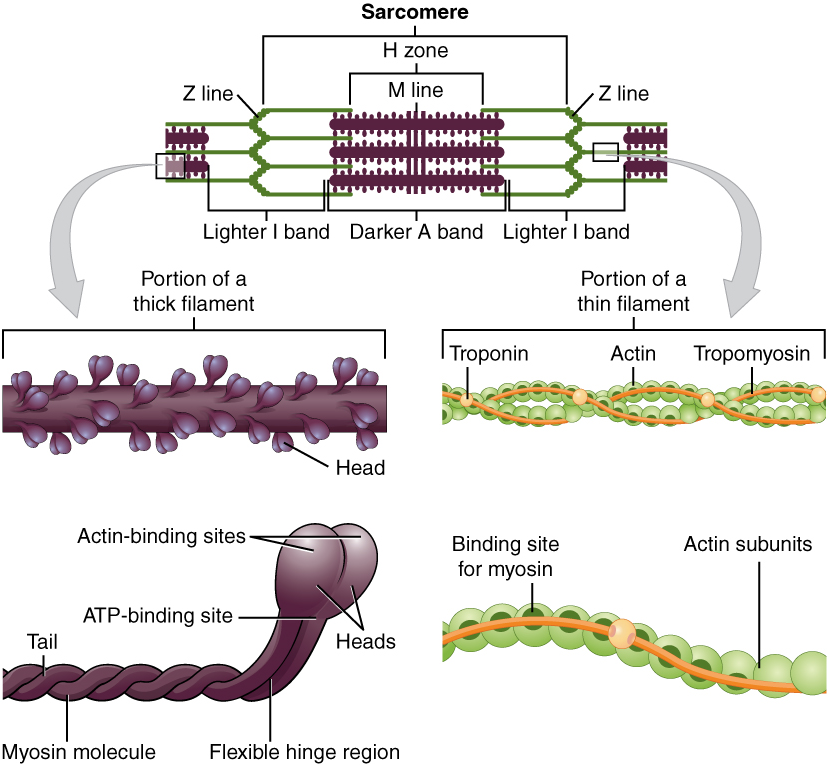
The Sarcomere: The striated appearance of skeletal muscle fibers is due to the arrangement of the myofilaments of actin and myosin in sequential order from one end of the muscle fiber to the other. Each packet of these microfilaments and their regulatory proteins, troponin and tropomyosin (along with other proteins) is called a sarcomere.


The sarcomere is the functional unit of the muscle fiber. The sarcomere itself is bundled within the myofibril that runs the entire length of the muscle fiber and attaches to the sarcolemma at its end. As myofibrils contract, the entire muscle cell contracts. Because myofibrils are only approximately 1.2 μm in diameter, hundreds to thousands (each with thousands of sarcomeres) can be found inside one muscle fiber.
Each sarcomere is around 2 μm in length with a cylinder-like arrangement and is bordered by structures called Z-discs (also called Z lines, because pictures are two-dimensional), to which the actin myofilaments are anchored (Figure 13.4). Because the actin and its troponin-tropomyosin complex (projecting from the Z-discs toward the center of the sarcomere) form strands that are thinner than the myosin, it is called the thin filament of the sarcomere. Likewise, because the myosin strands and their multiple heads (projecting from the center of the sarcomere, toward but not all the way to, the Z-discs) have more mass and are thicker, they are called the thick filament of the sarcomere.
Test Your Knowledge
I. Describe the levels of muscle organization: fascia, fascicles, muscle fibers.
II. Describe the following structures of a muscle cell: sarcolemma, sarcoplasm, nuclei, mitochondria, sarcoplasmic reticulum, transverse tubules, myofibrils, myofilaments, sarcomere.
- Define the following terms:
- Fascia
- Fascicle
- Epimysium
- Perimysium
- Endomysium
- Muscle fiber
- Muscle cell
- Tendon
- Explain why skeletal muscle fibers appear to have striations.
- Describe the location and general structure of each of the following:
- Sarcolemma
- Sarcoplasm
- Sarcoplasmic reticulum
- Sarcomere
- Myofilaments
- Myofibrils
- Transverse tubules
III. Describe the following structures of a sarcomere: Z line, I band, A band, H zone, M line.
- Draw and fully label a diagram showing two adjacent, relaxed sarcomeres. Your diagram must include (labeled!):
- Z line
- I band
- A band
- H zone
- M line
- Sarcomere width
- Draw and fully label a diagram showing one fully contracted sarcomere. Your diagram must include labels:
- Z line
- I band
- A band
- H zone
- M line
- Sarcomere width
IV. Describe the basic structure of the thick and thin filaments and their primary protein components.
- Draw a diagram showing and identifying the major structural components of:
- A single myosin molecule
- A single thick filament
- A single thin filament
Part 2: Types of Body Movement
Synovial joints allow the body a tremendous range of movements. Each movement at a synovial joint results from the contraction or relaxation of the muscles that are attached to the bones on either side of the articulation. The type of movement that can be produced at a synovial joint is determined by four factors:
- Orientation of the muscle. Each muscle is attached at an origin and an insertion. The origin of the muscle is its attachment to the bone that will remain relatively stable when that muscle contracts. It is the bone to which the muscle is anchored. The other end of the muscle will be its insertion, which is its attachment to the bone which will move when that muscle contracts. The orientation of the muscle, which bone it is anchored to and which bone it inserts in, will determine the movement.
- Action of other muscles that may insert and/or originate on the same bone(s) that when any particular muscle contracts, the bone will be moved in a particular direction, different from the direction any single muscle may produce. It is not uncommon to see the same muscle being involved in two or more different movements.
- Type of joint between the bones. There are a number of different types of joints between bones. Only the synovial joint allows for any significant movement. Each specific joint is limited in the movement it can provide because of the shape of the ends of the bones in the joint and because of the tension in the ligaments holding the bones together.
- Muscle tension. This is a limitation that works in a similar manner to tension in the ligaments. An example of the role of muscle tension is demonstrated when touching one’s toes with the knees straight. The movement is restricted by the tension of the hamstring muscles.
While the ball-and-socket joint gives the greatest range of movement at an individual joint, in other regions of the body, several joints may work together to produce a particular movement. Overall, each type of synovial joint is necessary to provide the body with its great flexibility and mobility. There are many types of movement that can occur at synovial joints (Table 13.1). Movement types are generally paired, with one being the opposite of the other. Body movements are always described in relation to the anatomical position of the body: upright stance, with upper limbs to the side of body and palms facing forward.
| Type of Joint | Movement | Examples |
|---|---|---|
| Pivot | Uniaxial joint; allows rotational movement | Atlantoaxial joint (C1-C2 vertebrae articulation); proximal radioulnar joint |
| Hinge | Uniaxial joint; allows flexion/extension movements | Knee; elbow; ankle; interphalangeal joints of fingers and toes |
| Condyloid | Biaxial joint; allows flexion/extension, abduction/adduction, and circumduction movements | Metacarpophalangeal (knuckle) joints of fingers; radiocarpal joint of wrist; metatarsophalangeal joints of toes |
| Saddle | Biaxial joint; allows flexion/extension, abduction/adduction, and circumduction movements | First carpometacarpal joint (carpometacarpal joint of the thumb); sternoclavicular joint |
| Plane | Multiaxial joint; allows inversion/eversion of the foot, flexion/extension, and lateral flexion of the vertebral column | intertarsal joints of foot; superior-inferior articular process articulations between vertebrae |
| Ball-and-socket | Multiaxial joint; allows flexion/extension, abduction/adduction, circumduction, and medial/lateral rotation movements | Shoulder joint, hip joint |
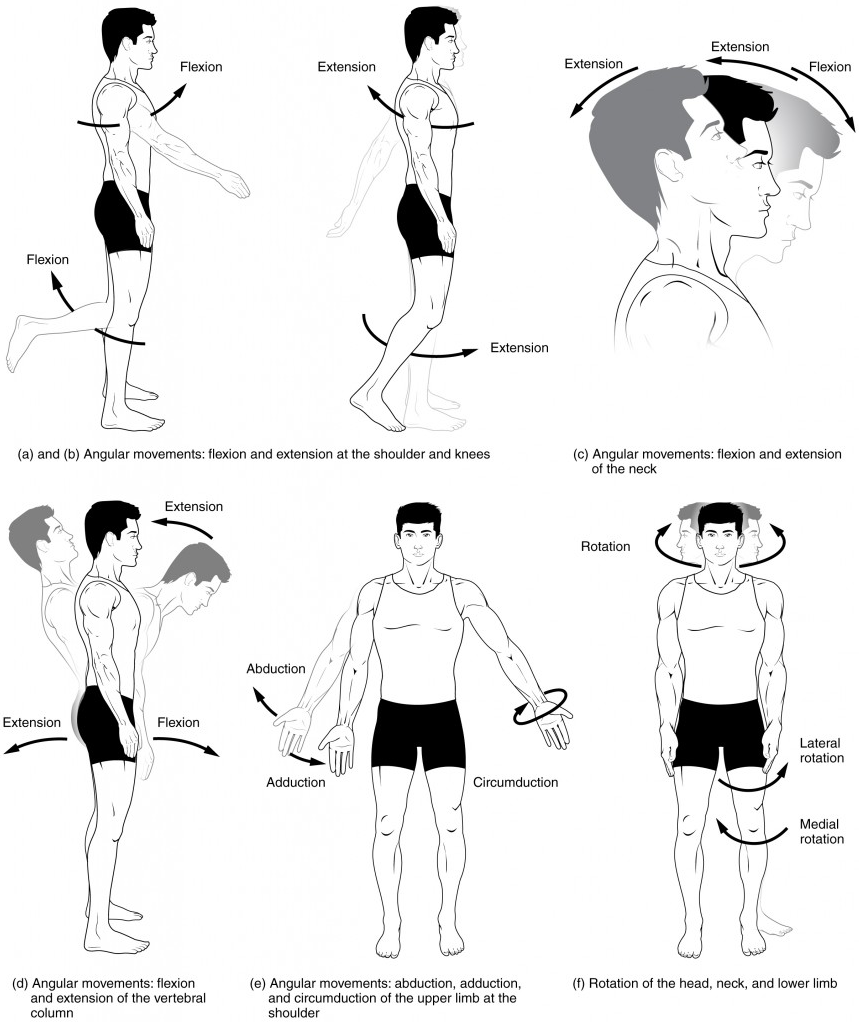
Flexion and Extension
Flexion and extension are movements that take place within the sagittal plane and involve anterior or posterior movements of the body or limbs. For the vertebral column, flexion (anterior flexion) is an anterior (forward) bending of the neck or body, while extension involves a posterior-directed motion, such as straightening from a flexed position or bending backward. Lateral flexion is the bending of the neck or body toward the right or left side. These movements of the vertebral column involve both the symphysis joint formed by each intervertebral disc, as well as the plane type of synovial joint formed between the inferior articular processes of one vertebra and the superior articular processes of the next lower vertebra.
In the limbs, flexion decreases the angle between the bones (bending of the joint), while extension increases the angle and straightens the joint. For the upper limb, all anterior-going motions are flexion, and all posterior-going motions are extension. These include anterior-posterior movements of the arm at the shoulder, the forearm at the elbow, the hand at the wrist, and the fingers at the metacarpophalangeal and interphalangeal joints. For the thumb, extension moves the thumb away from the palm of the hand, within the same plane as the palm, while flexion brings the thumb back against the index finger or into the palm. These motions take place at the first carpometacarpal joint. In the lower limb, bringing the thigh forward and upward is flexion at the hip joint, while any posterior-going motion of the thigh is extension. Note that extension of the thigh beyond the anatomical (standing) position is greatly limited by the ligaments that support the hip joint. Knee flexion is the bending of the knee to bring the foot toward the posterior thigh, and extension is the straightening of the knee. Flexion and extension movements are seen at the hinge, condyloid, saddle, and ball-and-socket joints of the limbs (Figure 13.5a–d).
Hyperextension
Hyperextension is the abnormal or excessive extension of a joint beyond its normal range of motion, thus resulting in injury. Similarly, hyperflexion is excessive flexion at a joint. Hyperextension injuries are common at hinge joints such as the knee or elbow. In cases of “whiplash” in which the head is suddenly moved backward and then forward, a patient may experience both hyperextension and hyperflexion of the cervical region.
Abduction and Adduction
Abduction and Adduction: Abduction and adduction motions occur within the coronal plane and involve medial-lateral motions of the limbs, fingers, toes, or thumb. Abduction moves the limb laterally away from the midline of the body, while adduction is the opposing movement that brings the limb toward the body or across the midline. For example, abduction is raising the arm at the shoulder joint, moving it laterally away from the body, while adduction brings the arm down to the side of the body. Similarly, abduction and adduction at the wrist moves the hand away from or toward the midline of the body. Spreading the fingers or toes apart is also abduction, while bringing the fingers or toes together is adduction. For the thumb, abduction is the anterior movement that brings the thumb to a 90° perpendicular position, pointing straight out from the palm. Adduction moves the thumb back to the anatomical position, next to the index finger. Abduction and adduction movements are seen at condyloid, saddle, and ball-and-socket joints (Figure 13.55e).
Circumduction
Circumduction is the movement of a body region in a circular manner, in which one end of the body region being moved stays relatively stationary, while the other end describes a circle. It involves the sequential combination of flexion, adduction, extension, and abduction at a joint. This type of motion is found at biaxial condyloid and saddle joints and at multiaxial ball-and-socket joints (Figure 13.5e).
Rotation
Rotation can occur within the vertebral column, at a pivot joint, or at a ball-and-socket joint. Rotation of the neck or body is the twisting movement produced by the summation of the small rotational movements available between adjacent vertebrae. At a pivot joint, one bone rotates in relation to another bone. This is a uniaxial joint, and thus rotation is the only motion allowed at a pivot joint. For example, at the atlantoaxial joint, the first cervical (C1) vertebra (atlas) rotates around the dens, the upward projection from the second cervical (C2) vertebra (axis). This allows the head to rotate from side to side as when shaking the head “no.” The proximal radioulnar joint is a pivot joint formed by the head of the radius and its articulation with the ulna. This joint allows for the radius to rotate along its length during pronation and supination movements of the forearm.
Rotation can also occur at the ball-and-socket joints of the shoulder and hip. Here, the humerus and femur rotate around their long axis, which moves the anterior surface of the arm or thigh either toward or away from the midline of the body. Movement that brings the anterior surface of the limb toward the midline of the body is called medial (internal) rotation. Conversely, rotation of the limb so that the anterior surface moves away from the midline is lateral (external) rotation (Figure 13.5f). Be sure to distinguish medial and lateral rotation, which can only occur at the multiaxial shoulder and hip joints, from circumduction, which can occur at either biaxial or multiaxial joints.
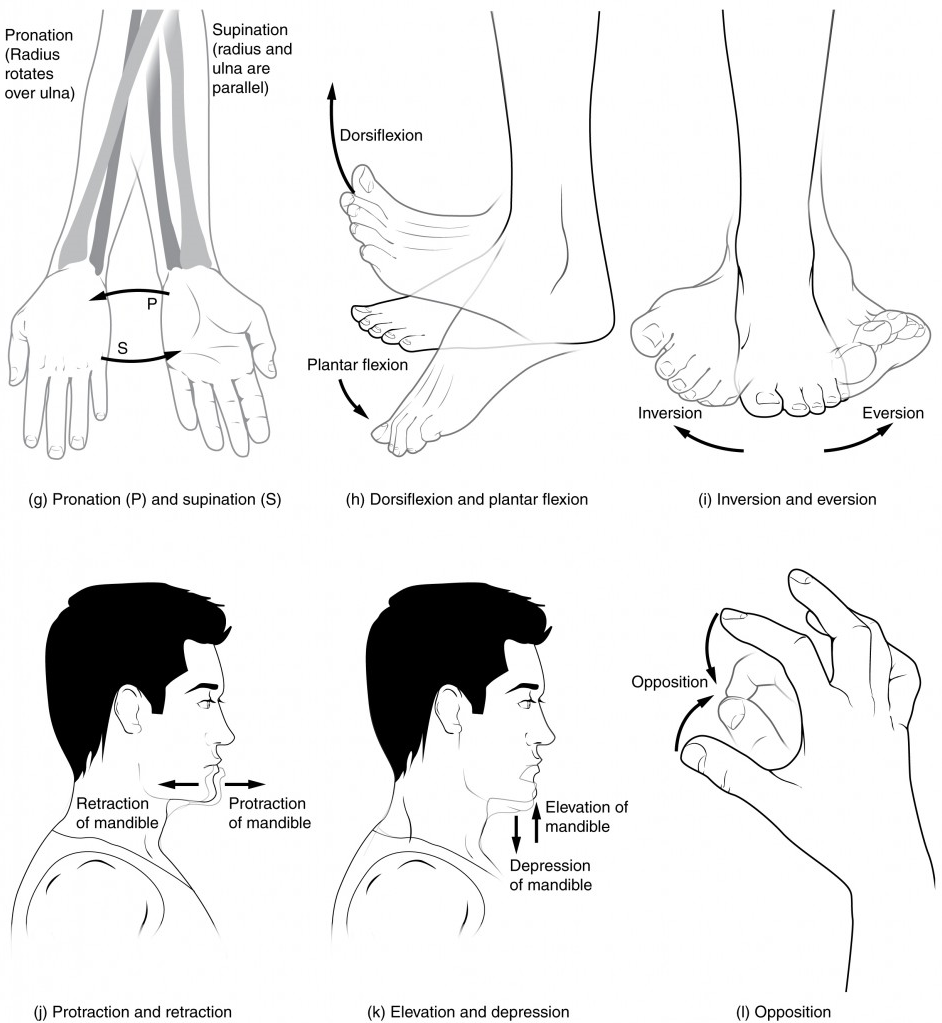
Supination and Pronation
Supination and pronation are movements of the forearm. In the anatomical position, the upper limb is held next to the body with the palm facing forward. This is the supinated position of the forearm. In this position, the radius and ulna are parallel to each other. When the palm of the hand faces backward, the forearm is in the pronated position, and the radius and ulna form an X-shape.
Supination and pronation are the movements of the forearm that go between these two positions. Pronation is the motion that moves the forearm from the supinated (anatomical) position to the pronated (palm backward) position. This motion is produced by the rotation of the radius at the proximal radioulnar joint, accompanied by movement of the radius at the distal radioulnar joint. The proximal radioulnar joint is a pivot joint that allows for the rotation of the head of the radius. Because of the slight curvature of the shaft of the radius, this rotation causes the distal end of the radius to cross over the distal ulna at the distal radioulnar joint. This crossing over brings the radius and ulna into an X-shape position. Supination is the opposite motion, in which rotation of the radius returns the bones to their parallel positions and moves the palm to the anterior facing (supinated) position. It helps to remember that supination is the motion you use when scooping up soup with a spoon (Figure 13.6g).
Dorsiflexion and Plantar Flexion
Dorsiflexion and plantar flexion are movements at the ankle joint, which is a hinge joint. Lifting the front of the foot, so that the top of the foot moves toward the anterior leg is dorsiflexion, while lifting the heel of the foot from the ground or pointing the toes downward is plantar flexion. These are the only movements available at the ankle joint (Figure 13.6h).
Inversion and Eversion
Inversion and eversion are complex movements that involve the multiple plane joints among the tarsal bones of the posterior foot (intertarsal joints) and thus are not motions that take place at the ankle joint. Inversion is the turning of the foot to angle the bottom of the foot toward the midline, while eversion turns the bottom of the foot away from the midline. The foot has a greater range of inversion than eversion motion. These are important motions that help to stabilize the foot when walking or running on an uneven surface and aid in the quick side-to-side changes in direction used during active sports such as basketball, racquetball, or soccer (Figure 13.6i).
Protraction and Retraction
Protraction and retraction are anterior-posterior movements of the scapula or mandible. Protraction of the scapula occurs when the shoulder is moved forward, as when pushing against something or throwing a ball. Retraction is the opposite motion, with the scapula being pulled posteriorly and medially toward the vertebral column. For the mandible, protraction occurs when the lower jaw is pushed forward, to stick out the chin, while retraction pulls the lower jaw backward (Figure 13.6j).
Depression and Elevation
Depression and elevation are downward and upward movements of the scapula or mandible. The upward movement of the scapula and shoulder is elevation, while a downward movement is depression. These movements are used to shrug your shoulders. Similarly, elevation of the mandible is the upward movement of the lower jaw used to close the mouth or bite on something, and depression is the downward movement that produces the opening of the mouth (Figure 13.6k).
Test Your Knowledge
V. Specify four factors which determine the type of movement accomplished by a muscle.
- Define “origin” and “insertion” as these terms pertain to skeletal muscles.
- Describe how the locations of the origin(s) and insertion(s) of a skeletal muscle affect the movement produced when that muscle contracts.
- Describe one specific example of a skeletal muscle that participates in multiple different movements, and then explain how it is possible for a skeletal muscle to participate in multiple different movements.
- Describe how the movement produced by contraction of a skeletal muscle is influenced by the structure of a joint about which the muscle moves the bone on which it inserts.
- Describe how tension in ligaments, tendons, and skeletal muscles can limit the range of motion available when a skeletal muscle contracts.
VII. Describe, using specific examples, 16 types of movements characteristic of skeletal muscle contractions.
- Clearly define each of the following terms.
- Flexion
- Extension
- Rotation
- Circumduction
- Abduction
- Adduction
- Elevation
- Depression
- Protraction
- Retraction
- Eversion
- Inversion
- Plantar flexion
- Dorsiflexion
- Pronation
- Supination
- Clearly describe (including an example of the body part being moved) and distinguish between each of the following pairs of terms:
- Flexion and extension
- Adduction and abduction
- Eversion and inversion
- Protraction and retraction
- Rotation and circumduction
- Plantar flexion and dorsiflexion
- Elevation and depression
- Pronation and supination
Part 3: The Muscular System
Think about the things that you do each day—talking, walking, sitting, standing, and running. All of these activities require the movement of particular skeletal muscles. Skeletal muscles are even used during sleep. The diaphragm is a sheet of skeletal muscle that has to contract and relax for you to breathe day and night. If you recall from your study of the skeletal system and joints, body movement occurs around the joints in the body. The focus of this chapter is on skeletal muscle organization. The system to name skeletal muscles will be explained; in some cases, the muscle is named by its shape, and in other cases, it is named by its location or attachments to the skeleton. If you understand the meaning of the name of the muscle, often it will help you remember its location and/or function. This chapter also will describe how skeletal muscles are arranged to accomplish movement and how other muscles may assist or be arranged on the skeleton to resist or carry out the opposite movement. The actions of the skeletal muscles will be covered in a regional manner, working from the head down to the toes.
Naming Skeletal Muscles
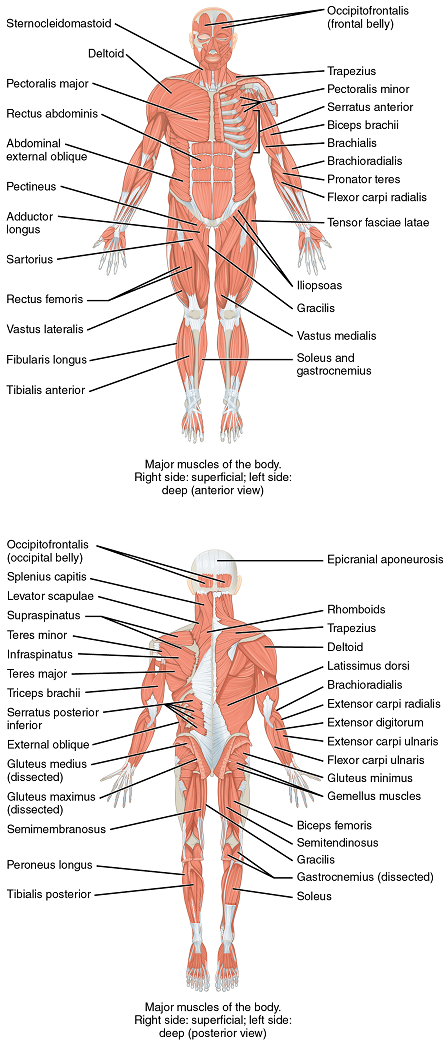
The Greeks and Romans conducted the first studies done on the human body in Western culture. The educated class of subsequent societies studied Latin and Greek, and therefore, the early pioneers of anatomy applied Latin and Greek terminology or roots when they named the skeletal muscles. The large number of muscles in the body and unfamiliar words can make learning the names of the muscles in the body seem daunting, but understanding the etymology can help. Etymology is the study of how the root of a particular word entered a language and how the use of the word evolved over time. Taking the time to learn the root of the words is crucial to understanding the vocabulary of anatomy and physiology (see Appendix II). When you understand the names of muscles, it will help you remember where the muscles are located and what they do (Figure 13.7, Table 13.2, Table 13.3, Table 13.4). Pronunciation of words and terms will take a bit of time to master, but after you have some basic information, the correct names and pronunciations will become easier.
| Example | Word | Latin Root 1 | Latin Root 2 | Meaning | Translation |
|---|---|---|---|---|---|
| abductor digiti minimi | abductor | ab = away from | duct = to move | moves away from | A muscle that moves the little finger/toe away |
| digiti | digitus = digit | refers to a finger or toe | |||
| minimi | minimus = minimal, tiny | little | |||
| adductor digiti minimi | adductor | ad = toward | duct = to move | moves toward | A muscle that moves the little finger/toe toward |
| digiti | digitus = digit | refers to a finger or toe | |||
| minimi | minimus = minimal, tiny | little |
Anatomists name the skeletal muscles according to a number of criteria, each of which describes the muscle in some way. These include naming the muscle after its shape, the direction of its muscle fibers, its size compared to other muscles in the area, its location in the body or the location of its attachments to the skeleton, how many origins it has, or its action. Often, a muscle’s name will refer to several of these characteristics (Table 13.3). You should be able to list the criteria and provide an example of each in the name of a muscle.
The shapes of some muscles are very distinctive, and the names, deltoid for the Greek letter delta (which looks like a triangle), reflect their shape. The direction of the muscle fibers and fascicles of a muscle can be used to name muscles by describing their orientation relative to the longitudinal axis of the body or of a limb, such as the rectus (straight) abdominis, or the oblique (at an angle) muscles of the abdomen.
For the buttocks, the size of the muscles influences the names: gluteus maximus (largest), gluteus medius (medium), and the gluteus minimus (smallest). Names are also given to muscles that indicate length—brevis (short) or longus (long). Some muscle names are used to indicate the number of muscles in a group. One example of this is the quadriceps, a group of four muscles located on the anterior (front) thigh.
The skeletal muscle’s anatomical location or its relationship to a particular bone often determines its name. Some muscles are named after their relative anatomical position: lateralis, medialis, dorsi (“dorsal”), anterior, and posterior.
The location of a muscle’s attachment can also appear in its name. When the name of a muscle is based on the attachments, the origin is always named first. For instance, the sternocleidomastoid muscle of the neck has a dual origin on the sternum (“sterno”) and clavicle (“cleido”) and inserts on the mastoid process of the temporal bone. Other muscle names can provide information as to how many origins a particular muscle has, such as the biceps brachii. The prefix bi indicates that the muscle has two origins, and tri indicates three origins.
The last feature by which to name a muscle is its action. When muscles are named for the movement they produce, one can find action words in their name.
|
Criteria |
Descriptions |
Meaning |
Example |
|---|---|---|---|
|
Shape |
Orbicularis |
Orbit (ring) |
Orbicularis oculi |
|
Deltoid |
Triangle |
Deltoid |
|
|
Orientation |
Rectus |
Straight |
Rectus femoris |
|
Oblique |
At an angle |
Abdominis external oblique |
|
|
Size |
Brevis |
Short |
Adductor brevis |
|
Longissimus/longus |
Long |
Adductor longus |
|
|
Maximus |
Largest |
Gluteus maximus |
|
|
Medius |
Medium |
Gluteus medius |
|
|
Minimus |
Smallest |
Gluteus minimus |
|
|
Anatomical position |
Medialis |
Medial (along the midline) |
Vastus medialis |
|
Lateralis |
Lateral (away from midline) |
Vastus lateralis |
|
|
Dorsi |
Dorsal (back) |
Latissimus dorsi |
|
|
Anterior |
Forward |
Tibialis anterior |
|
|
Posterior |
Rear |
Tibialis posterior |
|
|
Abdominis |
abdomen |
Abdominis external oblique |
|
|
Bone name |
various |
Rectus femoris (along femur) Frontalis (on top of frontal bone) |
|
|
Number of origins |
Bi-, tri- |
|
Biceps brachii |
|
Origin/Insertion location on skeleton |
Names of bones or parts of bones |
various |
Sternocleidomastoid (origins: sternum, clavicle; insertion: mastoid process) |
|
Actions |
Muscle actions |
|
Adductor longus |
| Example | Latin or Greek Translation | Mnemonic Device |
|---|---|---|
| ad- | to; toward | ADvance toward your goal |
| ab- | away from | Aliens ABduct you away from home |
| sub- | under | SUBmarines move underwater |
| -ductor | something that moves | A conDUCTOR makes a train move |
| anti- | against | If you are ANTIsocial, you are against engaging in social activities |
| epi- | on top of | She is the EPItome of goodness |
| apo- | to the side of | An APOstrophe separates parts of a contraction from each other |
| longissimus | longest | “Longissimus” is longer than the word “long” |
| longus | long | LONGus |
| brevis | short | BRief |
| maximus | large | MAXIMUm size |
| minimus | tiny; little | MINIMUm size |
| medius | between large and tiny | Of MEDIUm size |
| rectus | straight | A situation is considered RECTified when it is straightened out |
| multi | many | A rainbow is MULTIcoloured |
| uni- | one | A UNIcorn has one horn |
| bi- (Latin root) or di- (Greek root) | two | You can DIvide something into two pieces; BIcycles have two wheels |
| tri- | three | To TRIple your money, you multiply it by three |
| quad- | four | QUADruplets are four children born at one birth |
| externus | outside | EXTERNal |
| internus | inside | INTERNal |
Axial Muscles of the Head, Neck, and Back
The skeletal muscles are divided into two categories: axial (muscles of the trunk and head) and appendicular (muscles of the arms and legs). This system reflects the bones of the skeleton system, which are also arranged in this manner. The axial muscles are grouped based on location, function, or both. Some of the axial muscles may seem to blur the boundaries because they cross over to the appendicular skeleton. The first grouping of the axial muscles you will review includes the muscles of the head and neck, then you will review the muscles of the vertebral column, and finally you will review the oblique and rectus muscles.
Muscles That Move the Head: The head, attached to the top of the vertebral column, is balanced, moved, and rotated by the neck muscles. When these muscles act unilaterally, the head rotates. When they contract bilaterally, the head flexes or extends. The major muscle that laterally flexes and rotates the head is the sternocleidomastoid. In addition, both muscles working together are the flexors of the head. Place your fingers on both sides of the neck and turn your head to the left and to the right. You will feel the movement originate there. This muscle divides the neck into anterior and posterior triangles when viewed from the side (Figure 13.8).
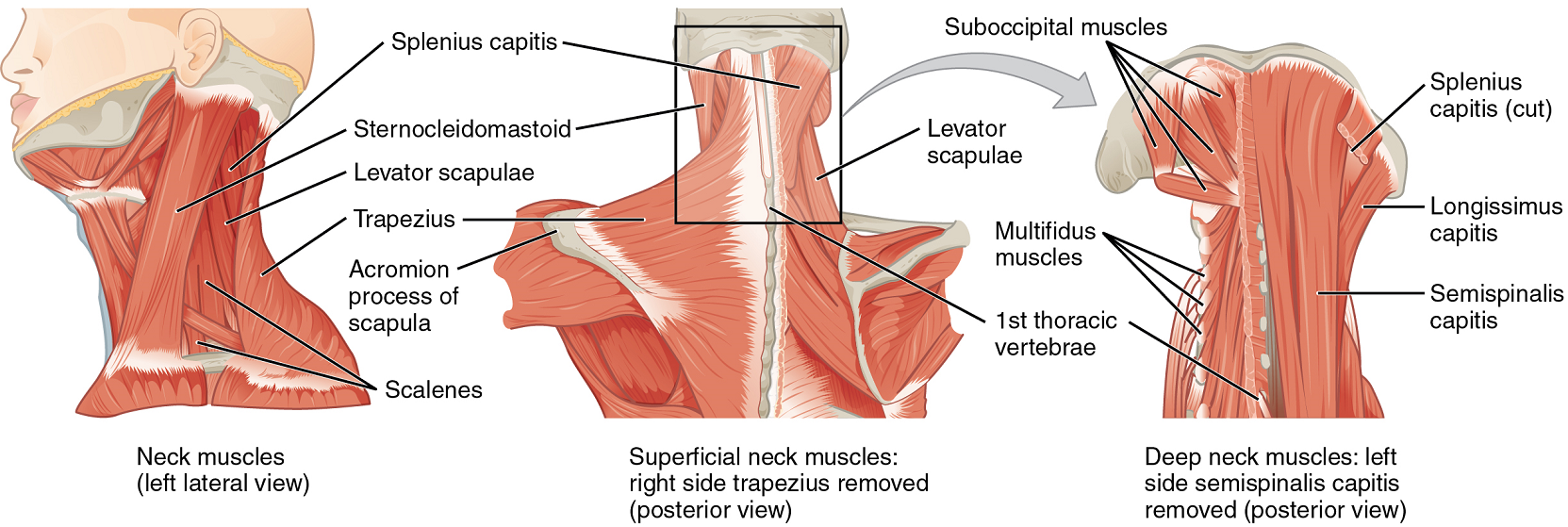
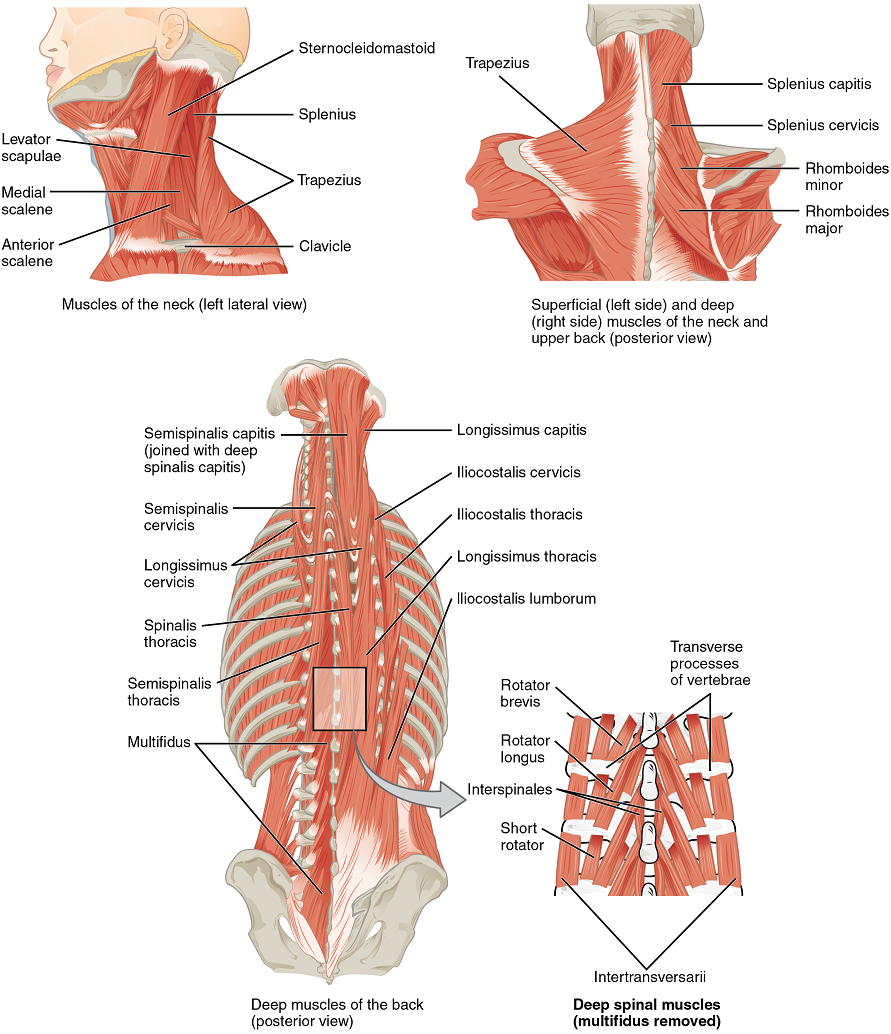
Muscles of the Posterior Neck and the Back: The posterior muscles of the neck are primarily concerned with head movements, like extension. The back muscles stabilize and move the vertebral column and are grouped according to the lengths and direction of the fascicles.
The erector spinae group forms the majority of the muscle mass of the back, and it is the primary extensor of the vertebral column. It controls flexion, lateral flexion, and rotation of the vertebral column and maintains the lumbar curve. The erector spinae comprises the iliocostalis (laterally placed) group, the longissimus (intermediately placed) group, and the spinalis (medially placed) group.
Muscles of the Abdominal Wall and Thorax
It is a complex job to balance the body on two feet and walk upright. The muscles of the vertebral column, thorax, and abdominal wall extend, flex, and stabilize different parts of the body’s trunk. The deep muscles of the core of the body help maintain posture as well as carry out other functions. The brain sends out electrical impulses to these various muscle groups to control posture by alternate contraction and relaxation. This is necessary so that no single muscle group becomes fatigued too quickly. If any one group fails to function, body posture will be compromised.
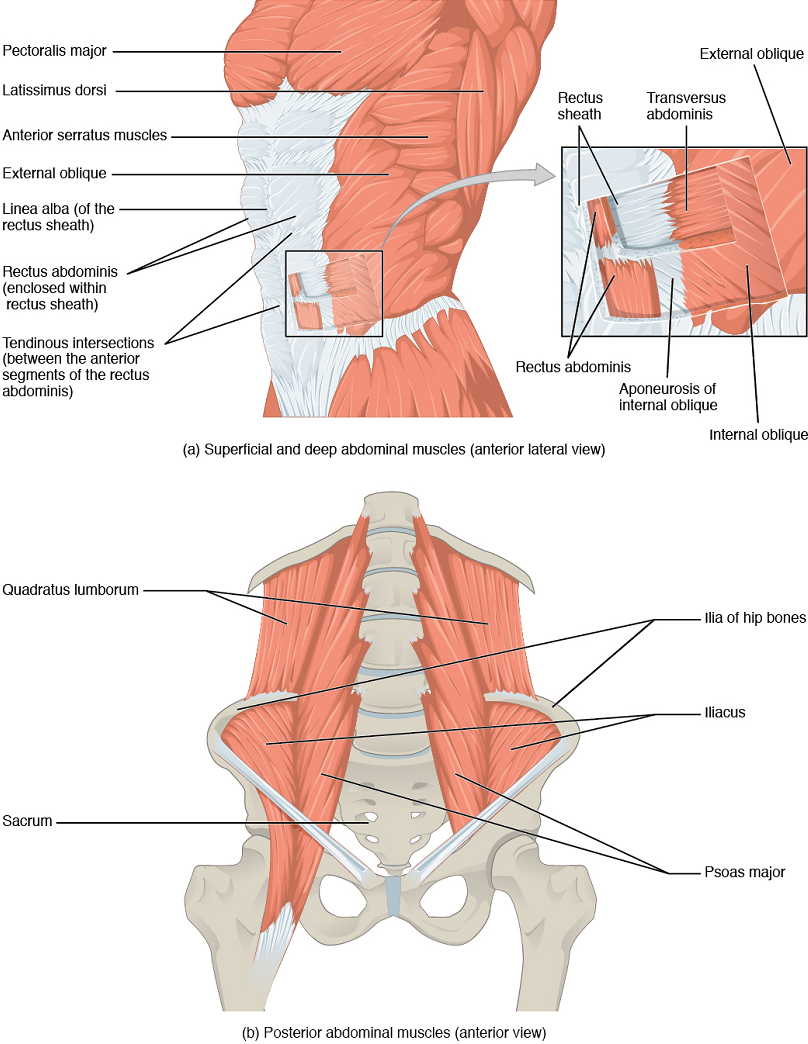
Muscles of the Abdomen: There are four pairs of abdominal muscles that cover the anterior and lateral abdominal region and meet at the anterior midline. These muscles of the anterolateral abdominal wall can be divided into four groups: the external obliques, the internal obliques, the transversus abdominis, and the rectus abdominis (Figure 13.10).
The external obliques, internal obliques, and transversus abdominis are three flat skeletal muscles in the antero-lateral wall of the abdomen. This arrangement of three bands of muscles in different orientations allows various movements and rotations of the trunk. The three layers of muscle also help to protect the internal abdominal organs in an area where there is no bone.
The linea alba is a white fibrous band that is made of the bilateral rectus sheaths that join at the anterior midline of the body. These enclose the rectus abdominis muscles (a pair of long, linear muscles, commonly called the “sit-up” muscles) that originate at the pubic crest and symphysis and extend the length of the body’s trunk to insert on the sternum and ribs five to seven. These muscles flex the abdomen, as in the motion or bending forward or doing a sit-up exercise. Each muscle is segmented by three transverse bands of collagen fibers called the tendinous intersections. This results in the look of “six-pack abs,” as each segment hypertrophies on individuals at the gym who do many sit-ups.
The posterior abdominal wall is formed by the lumbar vertebrae, parts of the ilia of the hip bones, psoas major and iliacus muscles, and quadratus lumborum muscle. This part of the core plays a key role in stabilizing the rest of the body and maintaining posture.
Muscles of the Thorax: The muscles of the chest facilitate breathing by changing the size of the thoracic cavity. When you inhale, your chest rises because the cavity expands. Alternately, when you exhale, your chest falls because the thoracic cavity decreases in size.
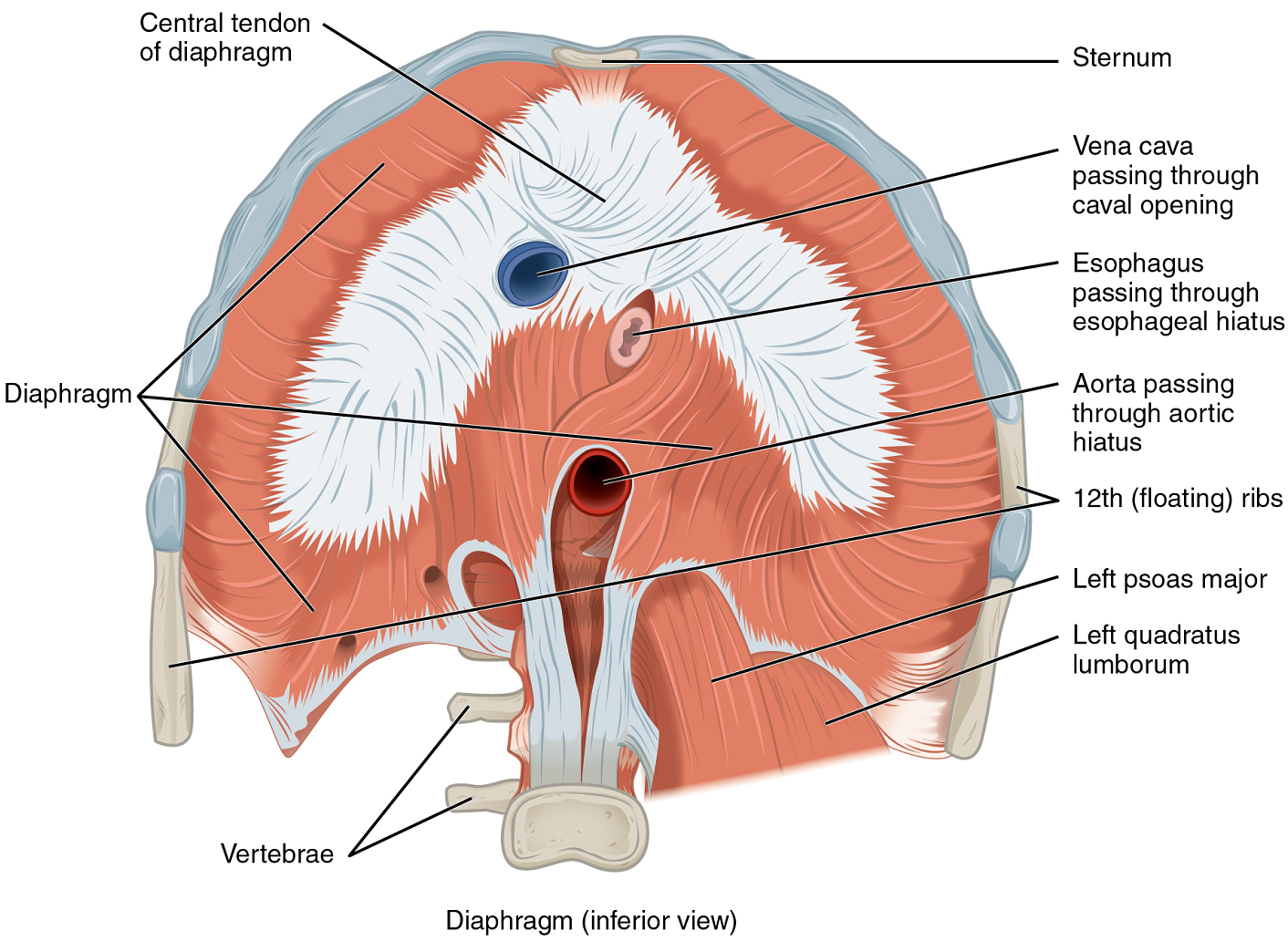
The Diaphragm: The change in volume of the thoracic cavity during breathing is due to the alternate contraction and relaxation of the diaphragm (Figure 13.11). It separates the thoracic and abdominal cavities, and is dome-shaped at rest. The superior surface of the diaphragm is convex, creating the elevated floor of the thoracic cavity. The inferior surface is concave, creating the curved roof of the abdominal cavity.
Defecating, urination, and even childbirth involve cooperation between the diaphragm and abdominal muscles (this cooperation is referred to as the “Valsalva maneuver”). You hold your breath by a steady contraction of the diaphragm; this stabilizes the volume and pressure of the peritoneal cavity. When the abdominal muscles contract, the pressure cannot push the diaphragm up, so it increases pressure on the intestinal tract (defecation), urinary tract (urination), or reproductive tract (childbirth).
The inferior surface of the pericardial sac and the inferior surfaces of the pleural membranes (parietal pleura) fuse onto the central tendon of the diaphragm. To the sides of the tendon are the skeletal muscle portions of the diaphragm, which insert into the tendon while having a number of origins including the xiphoid process of the sternum anteriorly, the inferior six ribs and their cartilages laterally, and the lumbar vertebrae and 12th ribs posteriorly.
The diaphragm also includes three openings for the passage of structures between the thorax and the abdomen. The inferior vena cava passes through the caval opening, and the esophagus and attached nerves pass through the esophageal hiatus. The aorta, thoracic duct, and azygous vein pass through the aortic hiatus of the posterior diaphragm.
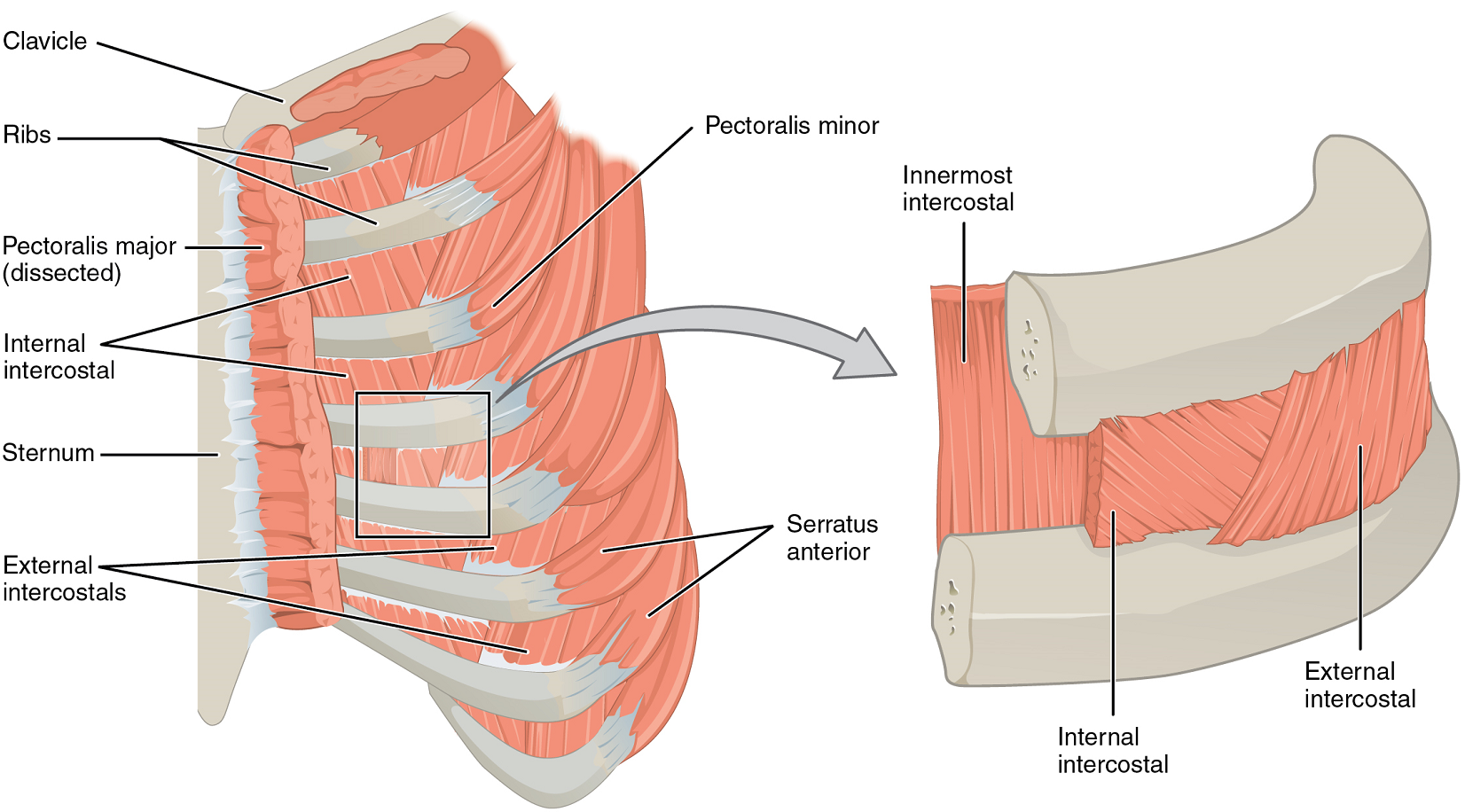
The Intercostal Muscles: There are three sets of muscles, called intercostal muscles, which span each of the intercostal spaces. The principal role of the intercostal muscles is to assist in breathing by changing the dimensions of the rib cage (Figure 13.12).
The 11 pairs of superficial external intercostal muscles aid in inspiration of air during breathing because when they contract, they raise the rib cage, which expands it. The 11 pairs of internal intercostal muscles, just under the externals, are used for expiration because they draw the ribs together to constrict the rib cage. The innermost intercostal muscles are the deepest, and they act as synergists for the action of the internal intercostals.
Muscles of the Pectoral Girdle and Upper Limbs
Muscles of the shoulder and upper limb can be divided into four groups: muscles that stabilize and position the pectoral girdle, muscles that move the entire arm, muscles that move the forearm, and muscles that move the wrists, hands, and fingers. The pectoral girdle, or shoulder girdle, consists of the lateral ends of the clavicle and scapula, along with the proximal end of the humerus, and the muscles covering these three bones to stabilize the shoulder joint. The girdle creates a base from which the head of the humerus, in its ball-and-socket joint with the glenoid fossa of the scapula, can move the arm in multiple directions.
Muscles that position the pectoral girdle are located either on the anterior thorax or on the posterior thorax (Figure 13.13). Among the most important of these is the trapezius, located in the posterior thorax that originate on the skull and upper vertebral column and insert on the clavicle and scapula. The trapezius is capable of diverse movements such as elevation and depression of the scapula (shrugging shoulders), moving the scapula together, and tilting the head backward.
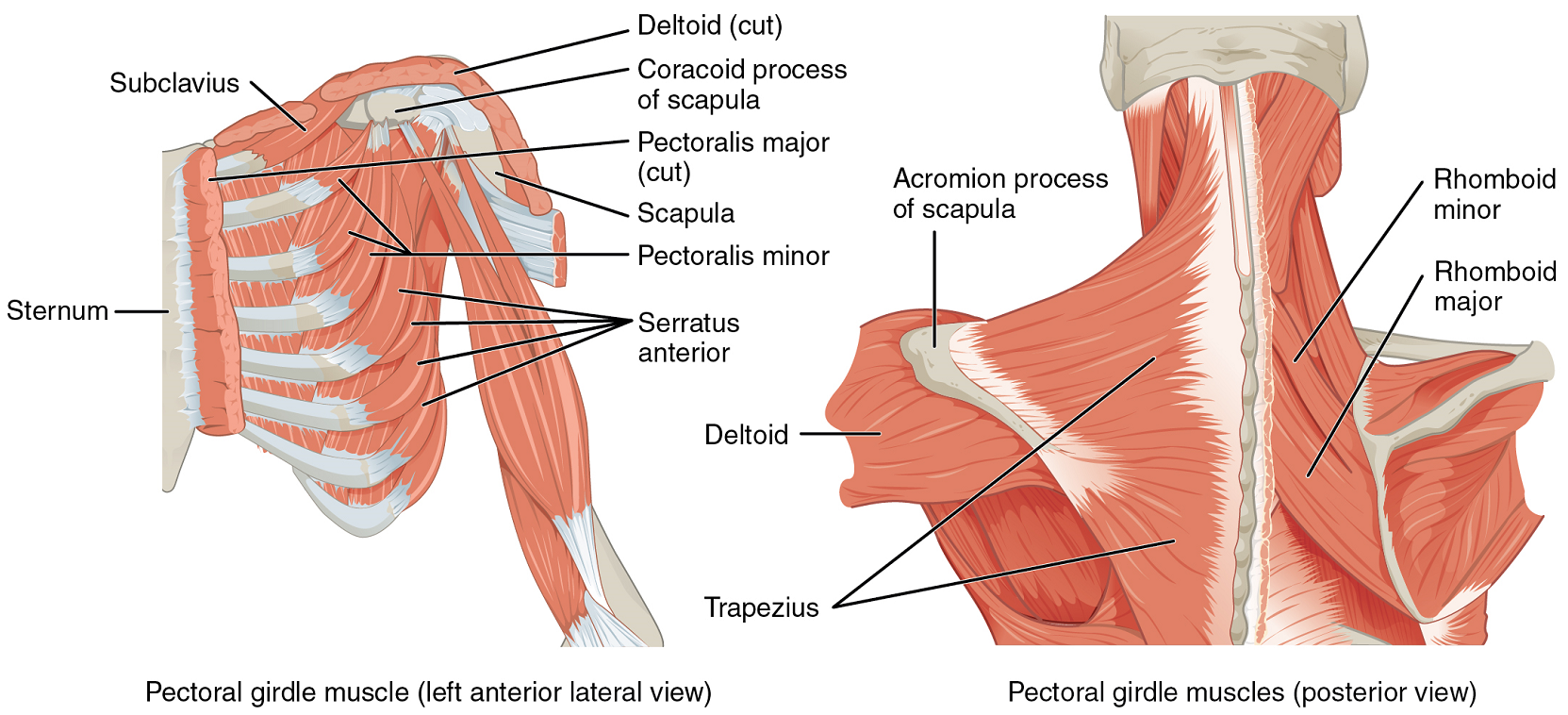
Muscles that move the humerus: Similar to the muscles that position the pectoral girdle, muscles that cross the shoulder joint and move the humerus bone of the arm include both axial and scapular muscles (Figure 13.14 and Table 13.5). The two axial muscles are the pectoralis major and the latissimus dorsi. The pectoralis major is thick and fan-shaped, covering much of the superior portion of the anterior thorax. The broad, triangular latissimus dorsi is located on the inferior part of the back, where it inserts into a thick connective tissue sheath called an aponeurosis.
The rest of the shoulder muscles originate on the scapula. The anatomical and ligamental structure of the shoulder joint and the arrangements of the muscles covering it allow the arm to carry out different types of movements. The deltoid, the thick muscle that creates the rounded lines of the shoulder, is the major abductor of the arm, but it also facilitates flexing and medial rotation, as well as extension and lateral rotation. Named for its location, the supraspinatus (superior to the spine of the scapula) abducts the arm. The thick and flat teres major extends the arm and assists in adduction and medial rotation of it. The long teres minor laterally rotates and extends the arm. Finally, the coracobrachialis flexes and adducts the arm (Table 13.5)
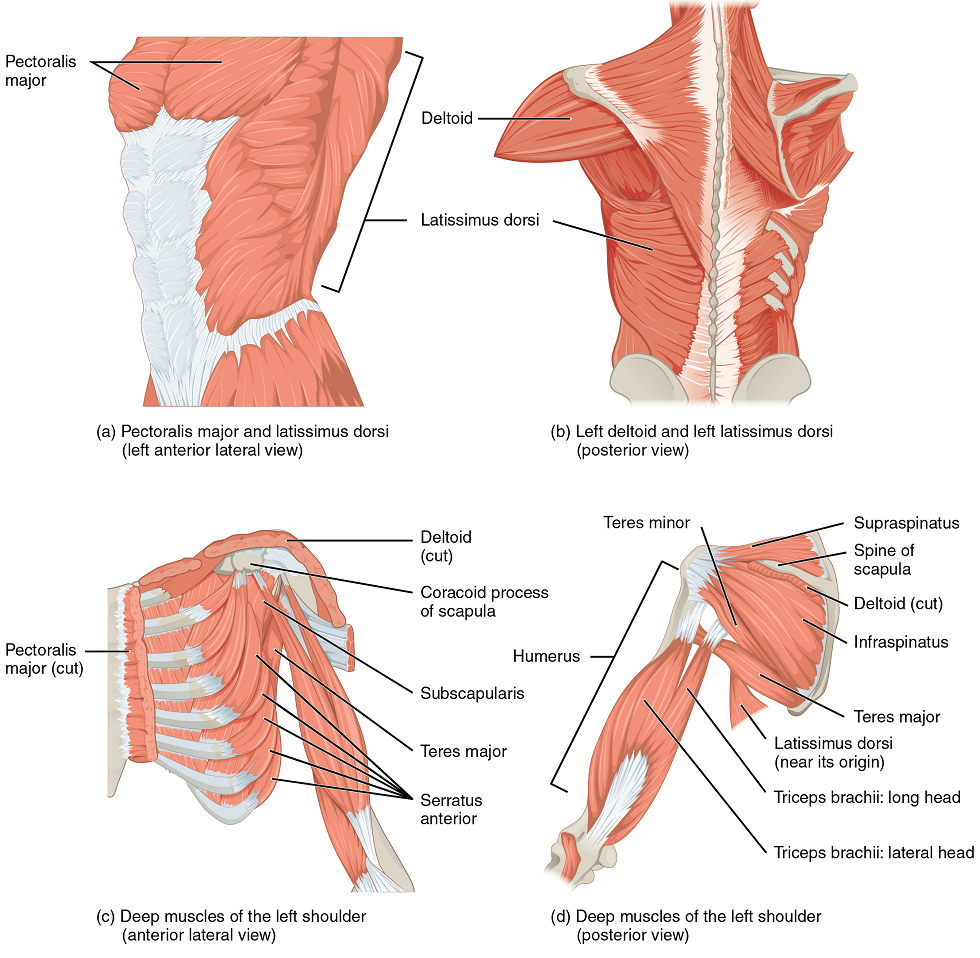
The tendons of the deep subscapularis, supraspinatus, infraspinatus, and teres minor connect the scapula to the humerus, forming the rotator cuff (musculotendinous cuff), the circle of tendons around the shoulder joint. When baseball pitchers undergo shoulder surgery, it is usually on the rotator cuff, which becomes pinched and inflamed and may tear away from the bone due to the repetitive motion of bringing the arm overhead to throw a pitch.
| Movement | Target | Target motion direction | Prime mover | Origin | Insertion |
|---|---|---|---|---|---|
| Axial muscles | |||||
|
Brings elbows together; moves elbow up (as during an uppercut punch) |
Humerus |
Flexion; adduction; medial rotation |
Pectoralis major |
Clavicle, sternum, cartilage of certain ribs (1–6 or 1–7); aponeurosis of external oblique muscle |
Greater tubercle of humerus |
|
Moves elbow back (as in elbowing someone behind you); spreads elbows apart |
Humerus, scapula |
Humerus:extension, adduction and medial rotation;
Scapula: depression |
Latissimus dorsi | Thoracic vertebrae (T7–T12); Lumbar vertebrae; lower ribs (9–12); iliac crest | Intertubercular sulcus of humerus |
| Scapular muscles | |||||
| Lifts arms at shoulder | Humerus | Abduction; flexion; extension; medial and lateral rotation | Deltoid | Trapezius; Clavicle; Acromion spine of scapula | Deltoid tuberosity of humerus |
| Rotates elbow outwards, as during a tennis swing | Humerus | Abduction | Supraspinatus | Supraspinous fossa of scapula | Greater tubercle of humerus |
| Rotate elbow outward | Humerus | Extension; Adduction | Teres major | Posterior surface of scapula | Intertubercular sulcus of humerus |
| Moves elbow up and across body, as when putting hand on chest. | Humerus | Flexion; adduction | Coracobrachialis | Coracoid process of scapula | Medial surface of humerus shaft |
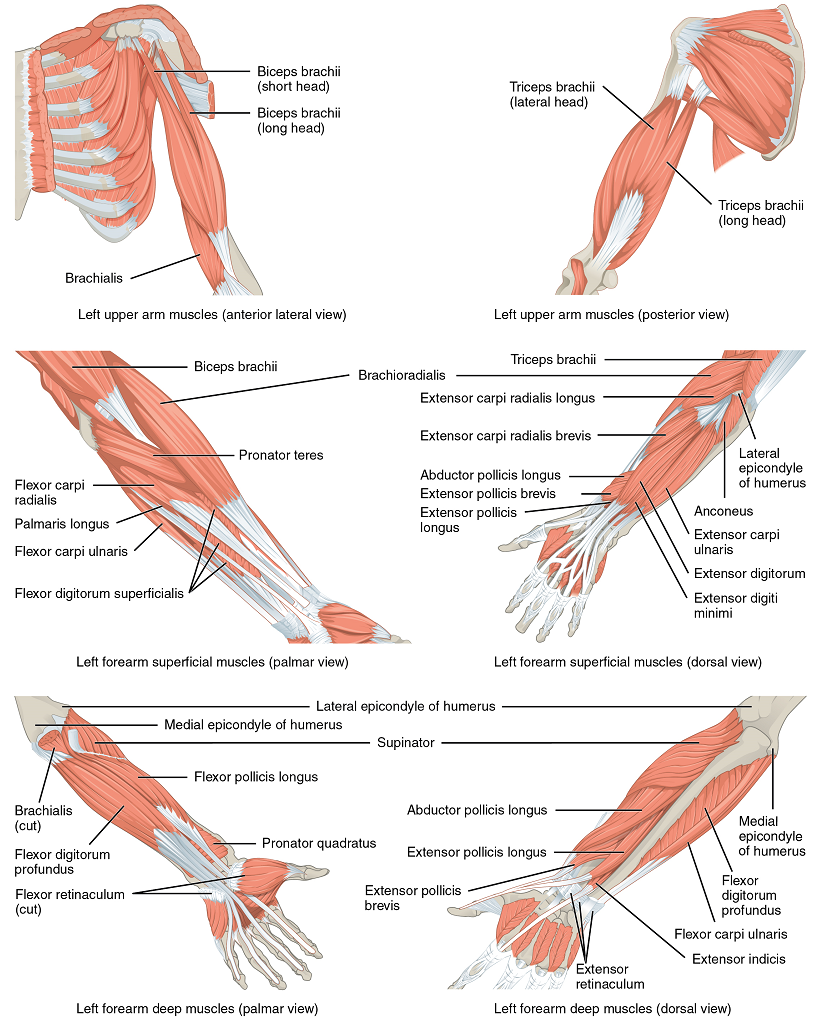
Muscles That Move the Forearm: The forearm, made of the radius and ulna bones, has four main types of action at the hinge of the elbow joint: flexion, extension, pronation, and supination. The forearm flexors include the biceps brachii and brachioradialis. The major extensor is the triceps brachii.
The biceps brachii and brachioradialis flex the forearm. The two-headed biceps brachii crosses the shoulder and elbow joints to flex the forearm, also taking part in supinating the forearm at the radioulnar joints and flexing the arm at the shoulder joint. The brachioradialis can flex the forearm quickly or help lift a load slowly. These muscles and their associated blood vessels and nerves form the anterior compartment of the arm (anterior flexor compartment of the arm; Figure 13.15 and Table 13.6).
| Movement | Target | Target motion direction | Prime mover | Origin | Insertion |
| Anterior muscles (flexion) | |||||
|
Performs a bicep curl; also allows palm of hand to point toward body while flexing |
Forearm |
Flexion; supination |
Biceps brachii |
Scapula: coracoid process and tubercle above glenoid cavity |
Radial tuberosity |
|
Assists and stabilizes elbow while performing a bicep curl |
Forearm |
Flexion | Brachioradialis | Lateral supracondylar ridge at distal end of humerus | Base of styloid process of radius |
| Posterior muscle (extension) | |||||
| Extends forearm, as during a punch | Forearm | Extension | Triceps brachii | Infraglenoid tubercle of scapula; posterior shaft of humerus; posterior humeral shaft distal to radial groove | Olecranon process of ulna |
Appendicular Muscles of the Pelvic Girdle and Lower Limbs
The appendicular muscles of the lower body position and stabilize the pelvic girdle, which serves as a foundation for the lower limbs. Comparatively, there is much more movement at the pectoral girdle than at the pelvic girdle. There is very little movement of the pelvic girdle because of its connection with the sacrum at the base of the axial skeleton. The pelvic girdle has less range of motion because its function is to stabilize and support the body.
Muscles of the Thigh: What would happen if the pelvic girdle, which attaches the lower limbs to the torso, were capable of the same range of motion as the pectoral girdle? For one thing, walking would expend more energy if the heads of the femurs were not secured in the acetabula of the pelvis. The body’s center of gravity is in the area of the pelvis. If the center of gravity were not to remain fixed, standing up would be difficult as well. Therefore, what the leg muscles lack in range of motion and versatility, they make up for in size and power, facilitating the body’s stabilization, posture, and movement.
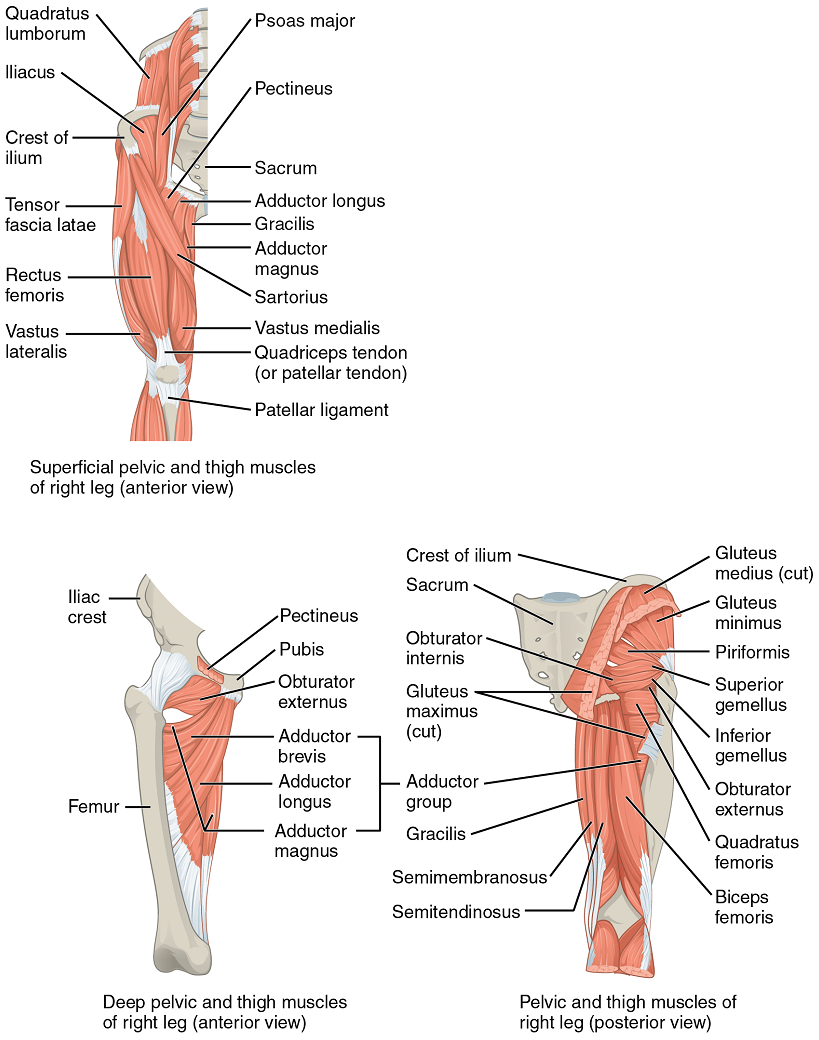
Gluteal Region Muscles That Move the Femur: Most muscles that insert on the femur (the thigh bone) and move it originate on the pelvic girdle. The psoas major and iliacus make up the iliopsoas group. Some of the largest and most powerful muscles in the body are the gluteal muscles or gluteal group. The gluteus maximus is the largest and deep to the gluteus maximus is the gluteus medius (Figure 13.16 and Table 13.7).
| Movement | Target | Target motion direction | Prime mover | Origin | Insertion |
| Iliopsoas group | |||||
|
Raises knee at hip, as if performing a knee attack; assists lateral rotators in twisting thigh (and lower leg) outward; assists with bending over, maintaining posture. |
Femur |
Thigh: flexion and lateral rotation; torso: flexion |
Psoas major Iliacus |
Psoas major: Lumbar vertebrae; and thoracic vertebra T12; Iliacus: iliac fossa, iliac crest and lateral sacrum |
Lesser trochanter of femur |
| Gluteal group | |||||
| Lowers knee and moves thigh back, as when getting ready to kick a ball | Femur | Extension | Gluteus maximus | Dorsal ilium; sacrum; coccyx | Gluteal tuberosity of femur; iliotibial tract |
| Opens thighs, as when doing a split | Femur | Abduction | Gluteus medius | Lateral surface of ilium | Greater trochanter of femur |
Thigh Muscles That Move the Femur, Tibia, and Fibula: Deep fascia in the thigh separates it into medial, anterior, and posterior compartments (Figure 13.16). The major muscle in the medial compartment of the thigh is the strap-like gracilis that adducts the thigh in addition to flexing the leg at the knee.
The muscles of the anterior compartment of the thigh flex the thigh and extend the leg. This compartment contains the quadriceps femoris group, which actually comprises four muscles that extend and stabilize the knee. The most important of these is the rectus femoris, located on the anterior aspect of the thigh. The tendon common to all four is the quadriceps tendon (patellar tendon), which inserts into the patella and continues below it as the patellar ligament. The patellar ligament attaches to the tibial tuberosity. In addition to the quadriceps femoris, the sartorius is a band-like muscle that extends from the anterior superior iliac spine to the medial side of the proximal tibia. This versatile muscle flexes the leg at the knee and flexes, abducts, and laterally rotates the leg at the hip. This muscle allows us to sit cross-legged.
The posterior compartment of the thigh includes muscles that flex the leg and extend the thigh. The three long muscles on the back of the knee are the hamstring group, which flexes the knee. These are the biceps femoris, semitendinosus, and semimembranosus. The tendons of these muscles form the popliteal fossa, the diamond-shaped space at the back of the knee.
Muscles That Move the Feet and Toes: Similar to the thigh muscles, the muscles of the leg are divided by deep fascia into compartments, although the leg has three: anterior, lateral, and posterior (Figure 13.17).
The muscles in the anterior compartment of the leg: the tibialis anterior, a long and thick muscle on the lateral surface of the tibia, the extensor hallucis longus, deep under it, and the extensor digitorum longus, lateral to it, all contribute to raising the front of the foot when they contract. The fibularis tertius, a small muscle that originates on the anterior surface of the fibula, is associated with the extensor digitorum longus and sometimes fused to it but is not present in all people. Thick bands of connective tissue called the superior extensor retinaculum (transverse ligament of the ankle) and the inferior extensor retinaculum hold the tendons of these muscles in place during dorsiflexion.
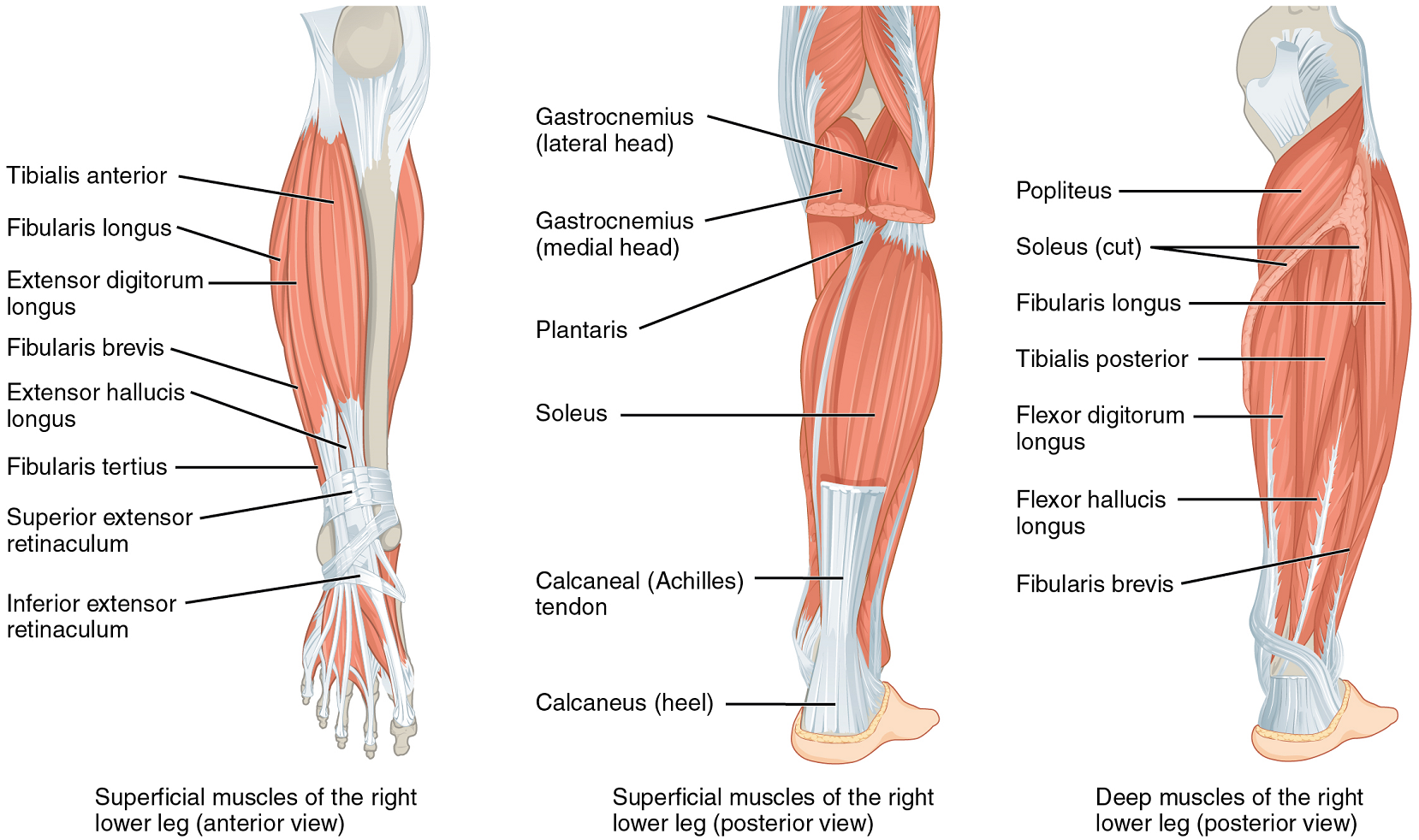
The lateral compartment of the leg includes two muscles: the fibularis longus (peroneus longus) and the fibularis brevis (peroneus brevis). The superficial muscles in the posterior compartment of the leg all insert onto the calcaneal tendon (Achilles tendon), a strong tendon that inserts into the calcaneal bone of the ankle. The muscles in this compartment are large and strong and keep humans upright. The most superficial and visible muscle of the calf is the gastrocnemius. Deep to the gastrocnemius is the wide, flat soleus. The plantaris runs obliquely between the two; some people may have two of these muscles, whereas no plantaris is observed in about seven percent of other cadaver dissections. The plantaris tendon is a desirable substitute for the fascia lata in hernia repair, tendon transplants, and repair of ligaments. There are four deep muscles in the posterior compartment of the leg as well: the popliteus, flexor digitorum longus, flexor hallucis longus, and tibialis posterior.
Test Your Knowledge
VI. Specify some of the criteria used in the naming of muscles.
- List, and provide an example for each of, at least seven criteria used to name skeletal muscles.
VII. Describe, using specific examples, 16 types of movements characteristic of skeletal muscle contractions.
- For each of the angular movement terms listed below, describe in detail at least one specific example of each in the human body. Each example should include the correct anatomical names for the agonist(s), antagonist(s), and joint(s) involved, as well as the origin(s) and insertion(s) of the muscles involved.
- Flexion
- Extension
- Abduction
- Adduction
- Plantarflexion
- Dorsiflexion
- For each of the complex movements listed below, describe in detail at least one specific example of each in the human body. Each example should include the correct anatomical names for the agonist(s), antagonist(s), and joint(s) involved, as well as the origin(s) and insertion(s) of the muscles involved.
- Rotation
- Circumduction
- Pronation
- Supination
- Eversion
- Inversion
- Elevation
- Depression
- Protraction
- Retraction
Practice
For the activity below, click the correct answer to each question.
Image Descriptions
Figure 13.1 image description: A comparison of three micrographs of the primary muscle tissues types: skeletal, smooth, and cardiac. All tissues were examined using a light microscope (LM) at the same magnification: 1600X. Skeletal and cardiac muscle are long and have prominent striations that are lacking in smooth muscle. Skeletal muscle fibers are arranged in parallel to one another, while cardiac muscle fibers are branched and interwoven like a basket. Smooth muscle cells are the smallest and least distinct of the three and have a delicate spindle shape, meaning they have tapered ends on both sides. [Return to image.]
Figure 13.2 image description: An illustration of the nested layers of connective tissues that form a skeletal muscle. A large muscle resembling a gastrocnemius connects to a bone via a tendon that is an extension of the outermost covering called the epimysium. A cross section reveals that the muscle is composed of multiple bundles called fascicles that are collectively bound together by the epimysium. Each fascicle is in turn wrapped by a layer called the perimysium. Inside the fascicle are the individual skeletal muscle cells, called fibers. Each fiber is enclosed by a layer called endomysium. Finally, each fiber is composed of fibrils. Although not labeled, the fibrils the contractile elements actin and myosin in addition to the labeled collagen. [Return to image.]
Figure 13.3 image description: A muscle fiber/cell is composed internally of many myofibrils and multiple nuclei externally. The entire muscle fiber is covered by a layer called the sarcolemma. Mitochondria are located amidst the microfibrils. The microfibrils are surrounded by a net-like sarcoplasmic reticulum and internally are composed of many thin (actin) and thick (myosin) filaments. These filaments are differentially arranged into specific regions of a contractile unit called a sarcomere. [Return to image.]
Figure 13.4 image description: A close-up representation of a sarcomere in muscle distinguishes the band/striations. The lighter/less-dense region, called the I Band, is formed exclusively by thin filaments (actin), while the darker/denser region called the A Band is filled with mostly thick filaments (myosin). A further close-up models myosin filaments as a thick rope sprouting multiple heads like golf clubs along its length. Each head is attached via a flexible neck and offers separate attachment regions for actin and myosin. On the other hand, the actin filament is modeled as a chain of bead-like elements containing a hollow binding site for the myosin head but surrounded by a thread-like molecule called tropomyosin. The tropomyosin appears to interfere with the access to the myosin binding location on the actin. Another component, called troponin, is associated with the tropomyosin but is not abundant. [Return to image.]
Figure 13.5 image description: This multi-part image shows different types of movements that are possible by different joints in the body. Labels read (from top, left): a and b angular movements: flexion and extension at the shoulders and knees; c) angular movements: flexion and extension of the neck (arrows pointing left and right to indicate movement). Labels (from bottom, left) read: d) angular movements: flexion and extension of the vertical column; e) angular movements abduction, adduction, and circumduction of the upper limb at the shoulder; f) rotation of the head, neck, and lower limb. [Return to image.]
Figure 13.6 image description: This multi-part image shows different types of movements that are possible by different joints in the body. Labels read (from top, left): g) pronation (P) and supination (S), h) dorsiflexion and plantar flexion, i) inversion and eversion. Labels read (from bottom, left): j) protraction and retraction, k) elevation and depression, and l) opposition. [Return to image.]
Figure 13.7 image description: This two-part diagram shows anterior (upper diagram) and posterior (lower diagram) views of the superficial muscle system. In the anterior view, different muscles are identified on the left and right side of the body, although all muscles are found on each side. Labels on the right side of the body read (from top to bottom): sternocleidomastoid, deltoid, pectoralis major, rectus abdominis, abdominal external oblique, pectineus, adductor longus, sartorius, rectus femoris, vastus lateralis, fibularis longus, and tibialis anterior. Labels for left side of the body read (from top to bottom): occipitofrontalis (frontal belly), trapezius, pectoralis minor, serratus anterior, biceps brachii, brachialis, brachioradialis, pronator teres, flexor carpi radialis, tensor fasciae latae, iliopsoas, gracilis, vastus medialis, soleus, and and gastrocnemius. As with the anterior view of muscles, the posterior view has different muscles identified on the left and right sides. Labels on the left side of the body read (from top to bottom): occipitofrontalis (occipital belly), splenius capitis, levator scapulae, supraspinatus, teres minor, intraspinatus, teres major, triceps brachii, serratus posterior inferior, external oblique, gluteus medius (dissected), gluteus maximus (dissected) semimembranosus, peroneus longus, and tibialis posterior. Labels for right side of the body read (from top to bottom): epicranial aponeurosis, rhomboids, trapezius, deltoid, latissimus dorsi, brachioradialis, extensor carpi radialis, extensor digitorum, extensor carpi ulnaris, flexor carpi ulnaris, gluteus minimus, gemellus muscles, biceps femoris, semitendinosus, gracilis, gastrocnemius (dissected), and soleus. [Return to image.]
Figure 13.8 image description: This three-part diagram shows the superficial (left and middle diagram) and deep neck muscles (right diagram). In the leftmost diagram, the superficial neck muscles are labeled on an illustration of the left lateral view of a neck. Labels read (from top to bottom): splenius capitis, sternocleidomastoid, levator scapulae, trapezius, and scalenes. In the middle diagram, the superficial neck muscles are viewed additionally from posterior view but with the right trapezius muscle removed to reveal more of these muscles. Labels read (from top to bottom): splenius capitis, sternocleidomastoid, levator scapulae, acromion process of scapula, and 1st thoracic vertebrae. The rightmost diagram shows the deep neck muscles from the posterior view and the semispinalis capitis removed from the left side. Labels read (from top to bottom): suboccipital muscles, splenius capitis (cut), longissimus capitis, semispinialis capitis, multifidus muscles, and 1st thoracic vertebrae. [Return to image.]
Figure 13.9 image description: This four-part diagram shows more neck muscles and back. The upper-left diagram shows the neck in the left lateral view. Labels read (from top to bottom): sternocleidomastoid, splenius, trapezius, levator scapulae, medial scalene, anterior scalene, clavicle. The upper-right diagram depicts the neck and upper back in posterior view; the trapezius muscle has been removed from the right side to show the deep neck muscles. Labels read (from top to bottom): splenius capitis, splenius cervicis, rhomboides minor, and rhomboides major. The bottom-left diagram shows the neck and back in posterior view. Deep muscle labels read (from top to bottom): semispinalis capitis (joined with deep spinalis capitis), longissimus capitis, semispinalis cervicis, iliocostalis cervicis, longissimus cervicis, illiocostalis thoracis, spinalis thoracis, longissimus thoracis, iliocostalis lumborum, and multifidus. The bottom-right diagram is an inset from the bottom-left diagram and shows the deepest spinal muscles with the multifidus removed. These muscle labels read (from top to bottom): rotator brevis, rotator longus, short rotator, interpspinales, and intertransversarii. [Return to image.]
Figure 13.10 image description: This two-part diagram shows anterior (upper diagram) and posterior (lower diagram) abdominal muscles. The anterior view labels read (from top to bottom): pectoralis major, latissimus dorsi, anterior serratus muscles, external oblique, linea alba (of the rectus sheath), rectus abdominis (enclosed within rectus sheath), and tendinous intersections (between the anterior segments of the rectus abdominis). An inset shows more detail of these abdominal muscles. Labels read (from top to bottom): external oblique, internal oblique, aponeurosis of internal oblique, transversus abdominis, rectus sheath, and rectus abdominis. In the posterior view, the following abdominal muscles are labeled to read (from top to bottom): quadratus lumborum, iliacus, and psoas major; also indicated are ilia of hip and sacrum bones. [Return to image.]
Figure 13.11 image description: An illustration of the diaphragm shows that it is a broad sheet-like muscle that spans attachments to the sternum, rib cage, and vertebral column. It contains openings to provide passage to blood vessels and the digestive tract. This inferior view has labels for the following muscles and openings read (from top to bottom): diaphragm, central tendon of diaphragm, vena cava passing through canal opening, esophagus passing through esophageal hiatus, aorta passing through aortic hiatus, left psoas major, and left quadratus lumborum. This view also has labels for the following bones (read from top to bottom): sternum, 12th (floating) ribs, and vertebrae. [Return to image.]
Figure 13.12 image description: The internal costal muscles are illustrated in this two-part diagram from the anterior perspective. The main left diagram shows the clavicle, sternum, and ribs along with labels for muscles read (from top to bottom): pectoralis major (dissected), internal intercostal, pectoralis major, and external intercostal. The right diagram is an inset from the left diagram and shows the striations and attachments of the intercostals more precisely. The deepest intercostal is labeled innermost intercostal and attaches to the opposite side (posterior) of the rib from the other superficial intercostals. The external intercostal is most superficial more lateral than the intermediate and more medial internal intercostal; the obliquely oriented fibers of these muscles are oriented perpendicularly to one another. [Return to image.]
Figure 13.13 image description: This two-part diagram shows the musculature associated with the supporting pectoral girdle. The left diagram shows the left pectoral girdle muscles from an anterior and lateral view. The labels read (from top to bottom): deltoid (cut), coracoid process of scapula, subclavius, pectoralis major (cut), scapula, pectoralis minor, and serratus anterior. The right diagram shows the posterior view of the pectoral girdle muscles. The labels read (from top to bottom): acromion process of scapula, deltoid, trapezius, rhomboid minor, rhomboid major, and trapezius. [Return to image.]
Figure 13.14 image description: This four-part diagram illustrates the superficial (upper diagram) and deep muscles (lower diagram) that move the humerus. The upper-left diagram shows an anterior lateral view, and the labels read (from top to bottom): pectoralis major and latissimus dorsi. The upper-right diagram shows the posterior view, and the labels read (from top to bottom): deltoid and latissimus dorsi. The bottom-left diagram shows an interior lateral view, and the labels read: deltoid (cut), coracoid process of scapula, pectoralis major (cut), subscapularis, teres major, and serratus anterior. The bottom-right diagram shows the posterior view, and the labels read (from top to bottom): supraspinatus, spine of scapula, deltoid (cut), infraspinatus, teres minor, teres major, latissimus dorsi (near its origin), humerus, triceps brachii: long head, and triceps brachii: lateral head. [Return to image.]
Figure 13.15 image description: This six-part illustration has three rows of images showing the muscles involved with the movement of the forearm. The top row shows images of the upper arm from anterior (left diagram) and poster (right diagram) views. The superficial (middle row) and deep (bottom row) of the forearm are also shown in palmar (left diagrams) and dorsal (right diagrams) views. In the top-left diagram, the labels read (from top to bottom): biceps brachii (short head), biceps brachii (long head), brachialis. The labels in the top-right diagram read (from top to bottom): triceps brachii (lateral head) and triceps brachii (long head). The middle-left diagram labels read (from top to bottom): biceps brachii, brachioradialis, pronator teres, flexor carpi radialis, palmaris longus, flexor carpi ulnaris, and flexor digitorum superficialis. The middle-right diagram labels read (from top to bottom): triceps brachii, brachioradialis, extensor carpi radialis longus, lateral epicondyle of humerus, anconeus, extensor carpi radialis brevis, abductor pollicis longus, extensor pollicis brevis, extensor pollicis longus, extensor carpi ulnaris, extensor digitorum, and extensor digiti minimi. The bottom-left diagram labels read (from top to bottom): lateral epicondyle of humerus, medial epicondyle of humerus, brachialis (cut), supinator, flexor digitorum profundus, flexor pollicis longus, pronator quadratus, and flexor retinaculum (cut). The bottom-right diagram labels read (from top to bottom): lateral epicondyle of humerus, medial epicondyle of humerus, supinator, abductor pollicis longus, flexor digitorum profundus, extensor pollicis longus, flexor carpi ulnaris, extensor indicis, and extensor retinaculum. [Return to image.]
Figure 13.16 image description: This three-part diagram shows the superficial (top diagram) and deep (bottom diagrams) muscles of the hip and thigh. The top diagram labels for the right pelvic and thigh muscles read (from top to bottom): quadratus lumborum, psoas major, iliacus, crest of ilium, sacrum, tensor fascia latae, adductor longus, gracilis, adductor magnus, sartorius, rectus femoris, vastus medialis, vastus lateralis, quadriceps tendon (or patellar tendon), and patellar ligament. The bottom-left diagram labels for the anterior view of the deep right pelvic and leg muscles read (from top to bottom): iliac crest, pectineus, pubus, obtrurator externus, adductor group (adductor brevis, adductor longus, adductor magnus), and femur. The bottom-right diagram for the posterior view of the deep right pelvic and leg muscles read: crest of ilium, gluteus medius (cut), sacrum, gluteus minimus, piriformis, superior gemellus, obtrurator internis, inferior gemellus, quadratus femoris, adductor group, gracilis, semimembranosus, and semitendinosus. [Return to image.]
Figure 13.17 image description: This three-part diagram shows the superficial (left and middle diagrams) and deep (right diagram) muscles of the lower leg. In an anterior view, the left diagram labels read: tibialis anterior, fibularus longus, extensor digitorum longus, fibularis brevis, extensor hallucis longus, fibularis tertius, superior extensor retinaculum, and inferior extensor retinaculum. The middle diagram labels for the deep muscles from a posterior view read (from top to bottom): gastrocnemius (lateral head), gastrocnemius (medial head), plantaris, soleus, calcaneal (Achilles) tendon, and calcaneus (heel). The right diagram labels for the posterior deep muscles read (from top to bottom): popliteus, soleus (cut), fibularis longus, tibialis posterior, flexor digitorum longus, flexor hallucis longus, and fibularis brevis. [Return to image.]
Ability to undergo neural stimulation.
Ability to stretch and rebound.
Ability to lengthen (extend).
Protein that makes up most of the thin myofilaments in a sarcomere muscle fibre.
Protein that makes up most of the thick cylindrical myofilament within a sarcomere muscle fiber.
Usually attached to bone, under voluntary control, each cell is a fiber that is multinucleated and striated.
Heart muscle, under involuntary control, composed of striated cells that attach to form fibres, each cell contains a single nucleus, contracts autonomously.
A multinucleate cell formed by the fusion of multiple cells or the division of nuclei.
Under involuntary control, moves internal organs, cells contain a single nucleus, are spindle-shaped, and do not appear striated; each cell is a fiber.
Steady state of body systems that living organisms maintain.
Nucleotide containing ribose and an adenine base that is essential in energy transfer.
Type of tissue that serves to hold in place, connect, and integrate the body’s organs and systems.
Loose and well-hydrated connective tissue covering each muscle fiber in a skeletal muscle.
Bundle of muscle fibres within a skeletal muscle
Connective tissue that bundles skeletal muscle fibers into fascicles within a skeletal muscle.
The most abundant of three protein fibres found in the extracellular matrix of connective tissues.
Fine fibrous protein, made of collagen subunits, which cross-link to form supporting “nets” within connective tissue.
Loose and well-hydrated connective tissue covering each muscle fibre in a skeletal muscle.
Fluid outside cells (plasma or interstitial fluid).
Dense regular connective tissue that attaches skeletal muscle to bone.
Fibrous membrane covering the outer surface of bone and continuous with ligaments.
Single process of the neuron that carries an electrical signal (action potential) away from the cell body toward a target cell.
Functional division of the nervous system that is concerned with conscious perception, voluntary movement, and skeletal muscle reflexes.
Band-like muscle that flexes, abducts, and laterally rotates the leg at the hip.
Plasma membrane of a skeletal muscle fiber.
Cytoplasm of a muscle cell.
Specialized smooth endoplasmic reticulum, which stores, releases, and retrieves Ca++.
Regulatory protein that binds to actin, tropomyosin, and calcium.
Regulatory protein that covers myosin-binding sites to prevent actin from binding to myosin.
Longitudinally, repeating functional unit of skeletal muscle, with all of the contractile and associated proteins involved in contraction.
Long, cylindrical organelle that runs parallel within the muscle fiber and contains the sarcomeres.
(Also Z-line) structure at the end of sarcomeres to which actin is anchored.
Joint at which the articulating surfaces of the bones are located within a joint cavity formed by an articular capsule.
End of a skeletal muscle that is attached to another structure (usually a bone) in a fixed position.
End of a skeletal muscle that is attached to the structure (usually a bone) that is moved when the muscle contracts.
Strong connective tissue bands that hold the bones at a moveable joint together.
Synovial joint at which the rounded portion of a bone rotates within a ring formed by a ligament and an articulating bone; functionally classified as uniaxial joint.
Movement that decreases the angle of a joint.
Movement that increases the angle of a joint.
Two-dimensional, vertical plane that divides the body or organ into right and left sides.
Describes the front or direction toward the front of the body; also referred to as ventral.
Describes the back or direction toward the back of the body; also referred to as dorsal.
Type of cartilaginous joint where the bones are joined by fibrocartilage.
Structure located between the bodies of adjacent vertebrae that strongly joins the vertebrae; provides padding, weight bearing ability, and enables vertebral column movements.
Synovial joint formed between the flattened articulating surfaces of adjacent bones; functionally classified as a multiaxial joint.
Describes a position below or lower than another part of the body proper; near or toward the tail (in humans, the coccyx, or lowest part of the spinal column); also referred to as caudal.
Describes a position above or higher than another part of the body proper; also referred to as cranial.
Synovial joint at which the convex surface of one bone articulates with the concave surface of a second bone; includes the elbow, knee, ankle, and interphalangeal joints; functionally classified as a uniaxial joint.
Synovial joint in which the shallow depression at the end of one bone receives a rounded end from a second bone or a rounded structure formed by two bones; found at the metacarpophalangeal joints of the fingers or the radiocarpal joint of the wrist; functionally classified as a biaxial joint.
Synovial joint in which the articulating ends of both bones are convex and concave in shape, such as at the first carpometacarpal joint at the base of the thumb; functionally classified as a biaxial joint.
Circular motion of the arm, thigh, hand, thumb, or finger that is produced by the sequential combination of flexion, abduction, extension, and adduction.
Movement in the coronal plane that moves a limb medially toward or across the midline of the body; bringing fingers together.
Movement in the coronal plane that moves a limb laterally away from the body; spreading of the fingers.
Type of diarthrosis; a joint that allows for movements within two planes (two axes).
Type of diarthrosis; a joint that allows for movements within three planes (three axes).
Movement of a bone around a central axis (atlantoaxial joint) or around its long axis (proximal radioulnar joint; shoulder or hip joint); twisting of the vertebral column resulting from the summation of small motions between adjacent vertebrae.
Synovial joint at which the rounded portion of a bone rotates within a ring formed by a ligament and an articulating bone; functionally classified as uniaxial joint.
Type of diarthrosis; joint that allows for motion within only one plane (one axis).
First cervical (C1) vertebra.
Bony projection (odontoid process) that extends upward from the body of the C2 (axis) vertebra.
Second cervical (C2) vertebra.
Bone located on the lateral side of the forearm.
Bone located on the medial side of the forearm.
Single bone of the upper arm.
Thigh bone; the single bone of the thigh.
Forearm motion that moves the palm of the hand from the palm backward to the palm forward position.
Forearm motion that moves the palm of the hand from the palm forward to the palm backward position.
Forearm position in which the palm faces backward.
Movement at the ankle that brings the top of the foot toward the anterior leg.
Foot movement at the ankle in which the heel is lifted off of the ground.
Foot movement involving the intertarsal joints of the foot in which the bottom of the foot is turned toward the midline.
Foot movement involving the intertarsal joints of the foot in which the bottom of the foot is turned laterally, away from the midline.
Anterior motion of the scapula or mandible.
Posterior motion of the scapula or mandible.
Shoulder blade bone located on the posterior side of the shoulder.
Unpaired bone that forms the lower jaw bone; the only moveable bone of the skull.
Downward (inferior) motion of the scapula or mandible.
Upward (superior) motion of the scapula or mandible.
Shoulder muscle that abducts the arm as well as flexes and medially rotates it and extends and laterally rotates it.
Straight
At an angle.
Largest
Short
Long
Four muscles that extend and stabilize the knee.
Major muscle that laterally flexes and rotates the head.
Large muscle mass of the back; primary extensor of the vertebral column.
Superficial abdominal muscle with fascicles that extend inferiorly and medially.
Flat, intermediate abdominal muscle with fascicles that run perpendicular to those of the external oblique.
Deep layer of the abdomen that has fascicles arranged transversely around the abdomen.
Long, linear muscle that extends along the middle of the trunk.
Long, linear muscle that extends along the middle of the trunk.
Flattened bone located at the center of the anterior chest.
Skeletal muscle that separates the thoracic and abdominal cavities and is dome-shaped at rest.
Hollowed or rounded inward, like the inside of a bowl. Opposite of convex.
Large systemic vein that returns blood to the heart from the inferior portion of the body.
Largest artery in the body, originating from the left ventricle and descending to the abdominal region where it bifurcates into the common iliac arteries at the level of the fourth lumbar vertebra; arteries originating from the aorta distribute blood to virtually all tissues of the body.
Major lymph vessel draining lymph into the circulatory system (blood) at the left subclavian vein.
Originates in the lumbar region and passes through the diaphragm into the thoracic cavity on the right side of the vertebral column; drains blood from the intercostal veins, esophageal veins, bronchial veins, and other veins draining the mediastinal region; leads to the superior vena cava.
Superficial intercostal muscles that raise the rib cage.
Muscles the intermediate intercostal muscles that draw the ribs together.
The deepest intercostal muscles that draw the ribs together.
Shoulder girdle; the set of bones, consisting of the scapula and clavicle, which attaches each upper limb to the axial skeleton.
Collarbone; elongated bone that articulates with the manubrium of the sternum medially and the acromion of the scapula laterally.
Describes a position in a limb that is nearer to the point of attachment or the trunk of the body.
Muscle that stabilizes the upper part of the back.
Thick, fan-shaped axial muscle that covers much of the superior thorax.
Broad, triangular axial muscle located on the inferior part of the back.
Muscle that abducts the arm.
Muscle that extends the arm and assists in adduction and medial rotation of it.
Muscle that abducts the arm.
Muscle that originates on the anterior scapula and medially rotates the arm.
Muscle that laterally rotates the arm.
Muscle that laterally rotates and extends the arm.
Two-headed muscle that crosses the shoulder and elbow joints to flex the forearm while assisting in supinating it and flexing the arm at the shoulder.
Muscle that can flex the forearm quickly or help lift a load slowly.
Three-headed muscle that extends the forearm.
Hip girdle; consists of a single hip bone, which attaches a lower limb to the sacrum of the axial skeleton.
Muscle that, along with the iliacus, makes up the iliopsoas.
Muscle that, along with the psoas major, makes up the iliopsoas.
Muscle group consisting of iliacus and psoas major muscles that flexes the thigh at the hip, rotates it laterally, and flexes the trunk of the body onto the hip.
Muscle group that extends, flexes, rotates, adducts, and abducts the femur.
Largest of the gluteus muscles that extends the femur.
Muscle deep to the gluteus maximus that abducts the femur at the hip.
Muscle that adducts the thigh and flexes the leg at the knee.
Muscle deep to the gluteus maximus on the lateral surface of the thigh that laterally rotates the femur at the hip.
(Also, patellar tendon) tendon common to all four quadriceps muscles, inserts into the patella.
Extension of the quadriceps tendon below the patella.
Three long muscles on the back of the upper leg.
One of the hamstring muscles.
The medial of the three muscles comprising the hamstring group.
The medial of the three muscles that comprise the hamstrings group.
Most superficial muscle of the calf.
