John and Marcia Price College of Engineering
26 Reverse Total Shoulder Arthroplasty Alters the Resting Orientation of the Scapula
Peyton King; Jared Zitnay; Peter Chalmers; Robert Tashjian; and Heath Henninger
Faculty Mentor: Heath Henninger (Orthopaedics, College of Medicine and Biomedical Engineering, Mechanical Engineering, University of Utah)
INTRODUCTION
The shoulder has the largest range of motion of any joint in the human body and is crucial for performing activities of daily living. Multiple treatment options are available to patients with rotator cuff deficiency or osteoarthritis, including total shoulder arthroplasty (TSA) and reverse total shoulder arthroplasty (rTSA). The rTSA is now performed more frequently, as it provides range of motion recovery and pain reduction even in the setting of rotator cuff deficiency. However, in vivo shoulder kinematics are altered and highly variable following rTSA, and thus consistent rehabilitation protocols for rTSA patients have not been established, as it is currently unknown what is “correct” or optimal rTSA motion. The goal of this ongoing research is to analyze the altered kinematics following rTSA, and the specific goal of this study was to analyze changes in resting scapulothoracic pose. The primary objective was to evaluate the difference in scapulothoracic pose between healthy controls and functionally recovered rTSA patients (>52 weeks post-operative). A subset of the included patients had pre-operative data as well, which was used to evaluate the effect of rTSA surgery on scapulothoracic joint angles.
METHODS
Our laboratory previously collected biplane fluoroscopy and skin-marker motion capture data of rTSA patients and healthy control subjects (IRB 71782, 113015). For this study, post-operative (>52 weeks) scapulae (N = 18)1,2 were compared to healthy shoulders (N = 10) from patients >45 years old (O45)3. A subset of rTSA patients also had pre-operative data (N= 7), which was used to compare to post-operative data. Motion capture data were tracked to determine the 3D position and orientation of the anatomical landmarks of the scapula, humerus, and torso. From these landmarks, we constructed bone and body segment coordinate systems and recast the scapulae into the torso coordinate system to account for variability in torso posture between data collections. We then calculated joint rotation matrices and performed joint angle decomposition for each subject. The ISB recommended Y-X’-Z’’ Euler sequence was used to evaluate the elevation, protraction, and tilt of the scapula4. The right-hand-rule denoted positive rotations, but reverse sign convention was used for scapular upward elevation for ease of graphical interpretation. Joint angles between post-operative and healthy control subjects were compared using a two-sided independent t-test. Absolute values of the pre- and post-operative joint angles were compared using a one-sample t-test where zero difference denoted no change. Absolute values were used to evaluate the magnitude of the change, since individual subjects often had large positive or negative post-operative changes and averaging the directional joint angles would negate this variability. Statistical significance was set at p≤0.05.
RESULTS
When comparing the post-operative joint angles to healthy controls, mean protraction of the scapula was 7.2±10.1° lower in rTSA patients (i.e., rTSA scapulae were more retracted, p=0.029) (Fig. 1). While both the downward rotation and anterior tilt were slightly larger in rTSA patients neither reached statistical significance (p=0.399 and p=0.120, respectively). When analyzed as absolute values to evaluate the magnitude of change between pre- and post-operative rTSA patients, protraction of the scapula differed by 8.0±3.3° (p=0.001), while the downward elevation differed by 5.3±3.6° (p=0.008) and anterior tilt differed by 6.5±4.8° (p=0.011) (Fig. 2).
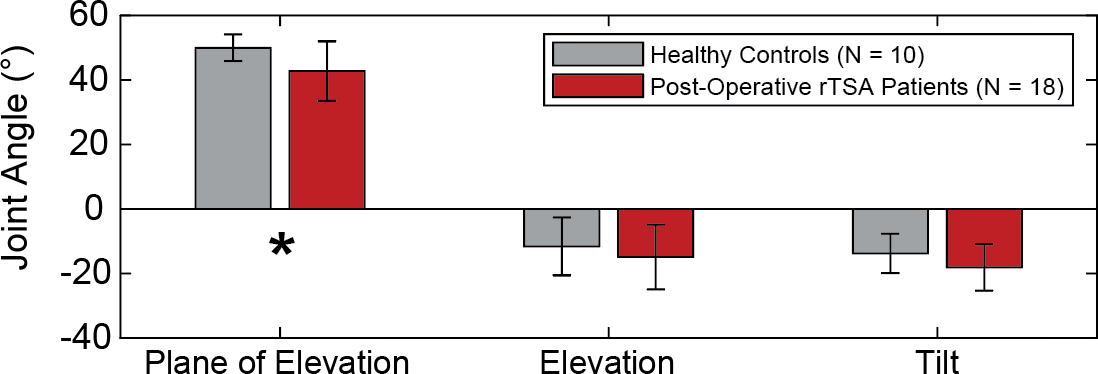
Figure 1. Healthy vs. post-operative rTSA joint angles. Mean±SD. * p≤0.05.
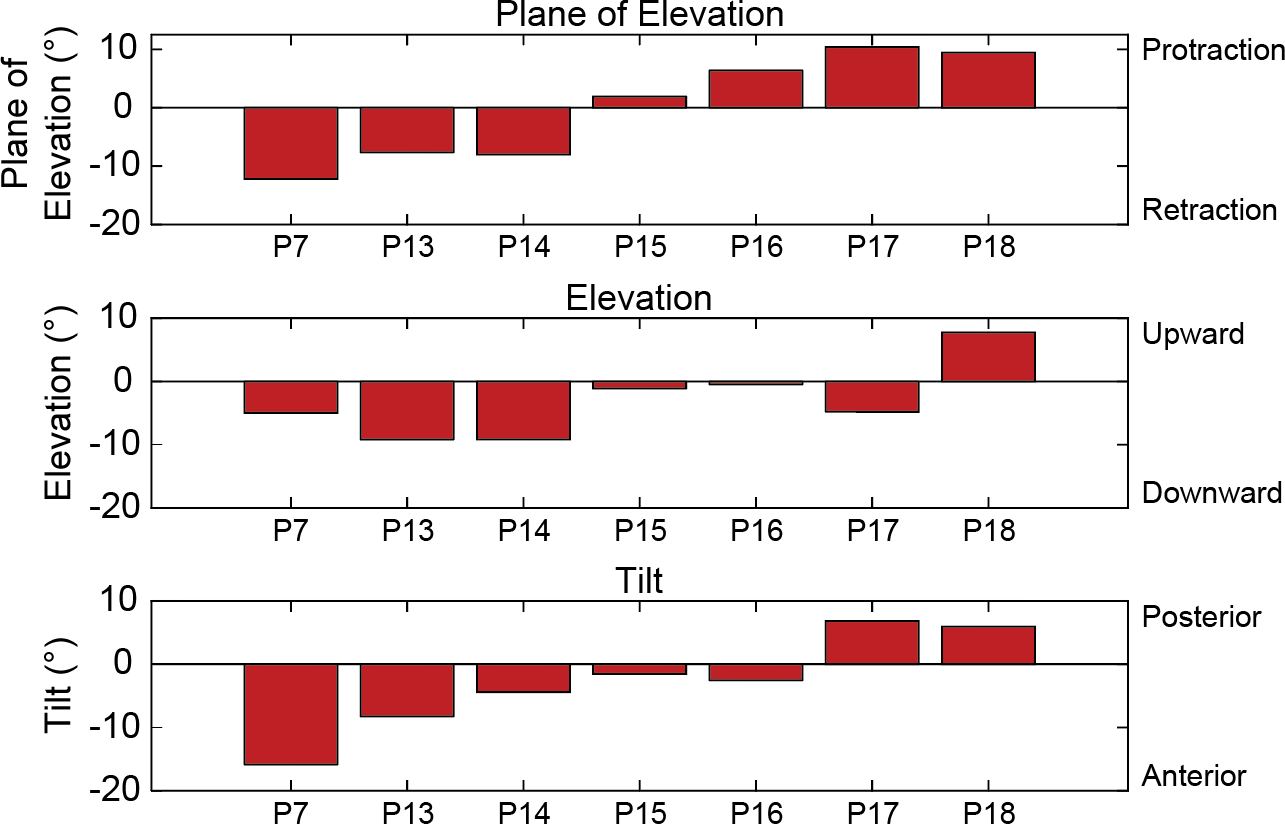
Figure 2. Difference from pre- to post-operative joint angles. Represented as post – pre.
DISCUSSION
The post-operative scapular pose after rTSA is less protracted (i.e., more retracted) than healthy control shoulders, whereas downward rotation and anterior tilt of the scapula did not differ. However, when analyzing the pre- to post-operative pose of patients, there was a large variation between subjects. The lack of a directional pattern in joint angles from pre- to post-operative suggests patients may recover with a large range of functional capabilities. The scapula and its stabilizing muscles adjust for the altered implant mechanics during recovery, resulting in these changes in joint angles. This result contrasts with our prior study5, which concluded that pre- to post-operative changes in scapulothoracic orientation were statistically insignificant. However, that study measured joint angles from 2D radiograph and did not control for variations in torso posture, while the present study used the true 3D pose of the scapula relative to the torso. Limitations of this study include small sample size and variations in subject age, pathology, and implant systems, but captures the variability inherent in rTSA patient populations.
SIGNIFICANCE
The changes in the scapular resting pose could affect how patients are able to perform activities of daily living, where scapular retraction could limit peak elevation and external rotation due to restricted ability to further retract the scapula during motion. Large variation in the recovery of each patient demonstrates the need for modifiable implant design and placement.
ACKNOWLEDGEMENTS
Funding was provided by the National Institute of Arthritis and Musculoskeletal and Skin Diseases (R01 AR067196).
REFERENCES
[1] Sulkar, HJ. Clin Orthop Relat Res, 2022, 480: 2254-65.
[2] Sulkar, HJ. J Shoulder Elbow Surg, 2022, 32: E133-44.
[3] Kolz, CW. J Biomech, 2021, 117: 110266.
[4] Wu, G. J Biomech, 2005, 38: 981-92.
[5] Kahn, TL. J Shoulder Elbow Surg, 2019, 28: E265- E270.
