Embryonic Development of the Respiratory System
Objective 11
Summarize the embryonic development of the respiratory system. Explain the role of surfactant in care of premature infants.
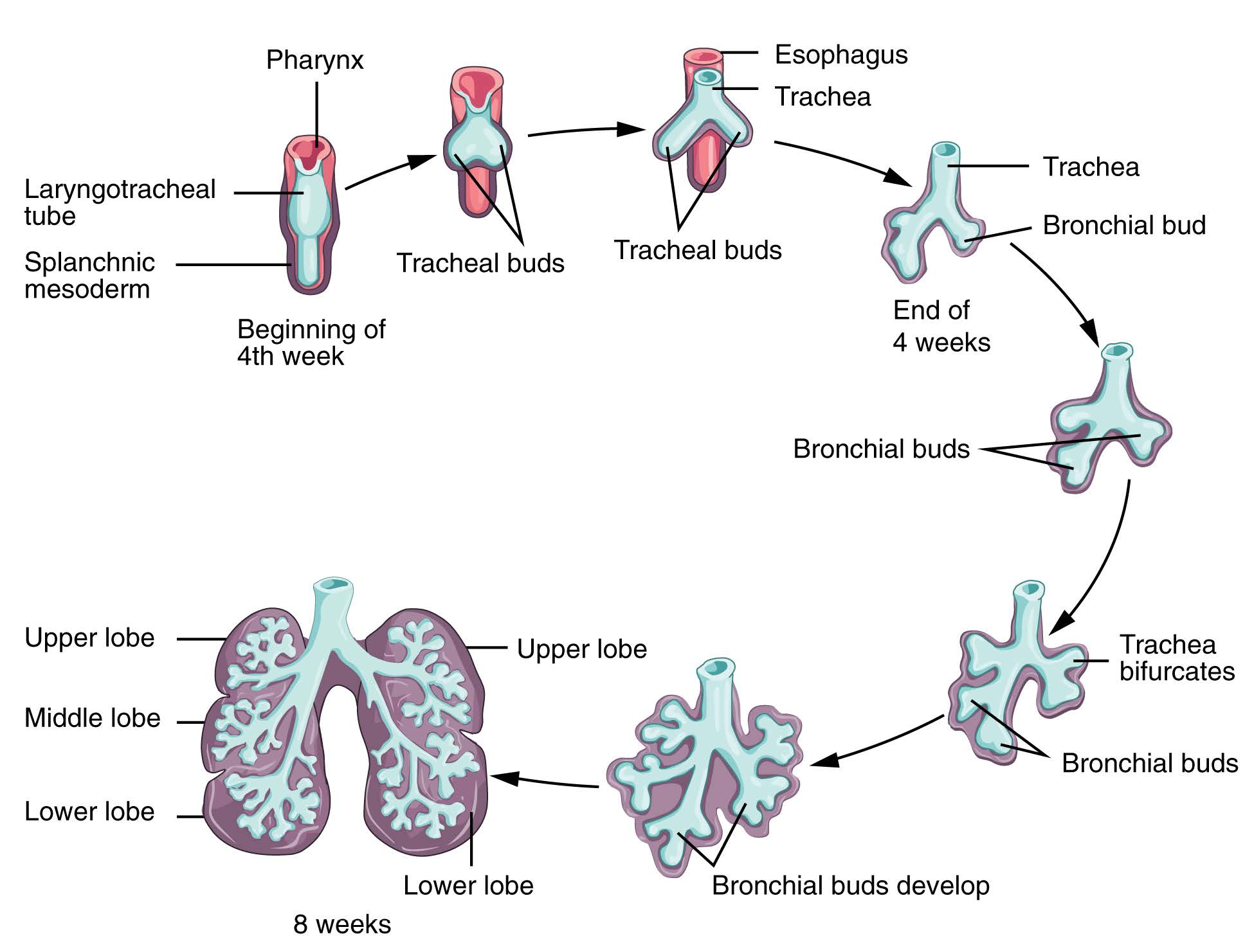
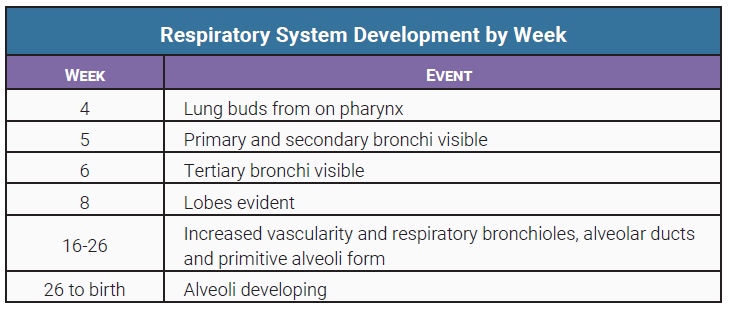
The lungs begin to develop during just the fourth week of pregnancy. At the fourth week, lungs begin to develop as buds on the pharynx. Then, the primary and secondary bronchi are visible at the fifth week. Tertiary bronchi at the sixth week. Lobes of the lung are evident at the end of the eighth week. At 16-26 weeks of pregnancy the lungs become highly vascular and respiratory bronchioles, alveolar ducts, and some primitive alveoli begin to develop. An infant born at 26 weeks may survive, however death frequently occurs because the respiratory system is so immature. From 26 weeks to birth, the alveoli develop. At birth, only about a sixth of the alveoli are present. These continue to develop during the first eight years of life.
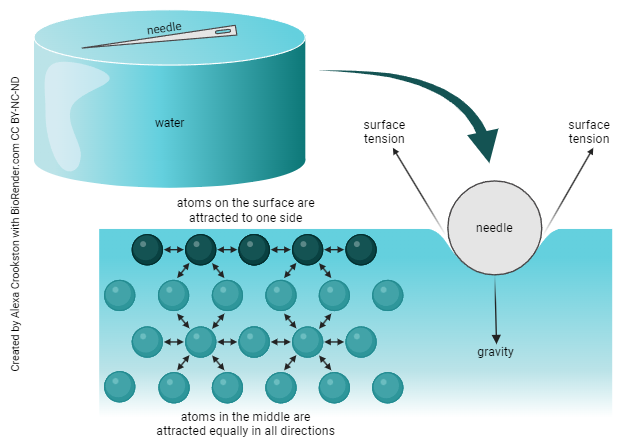
Remember from Unit 2 that water has surface tension. Hydrogen bonding tightly holds water molecules together. This is how you can pour water over the brim of your glass without it spilling over. Alveoli must overcome this surface tension to inflate.
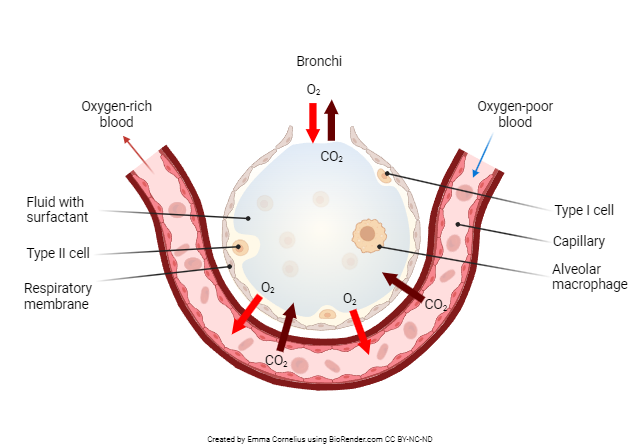
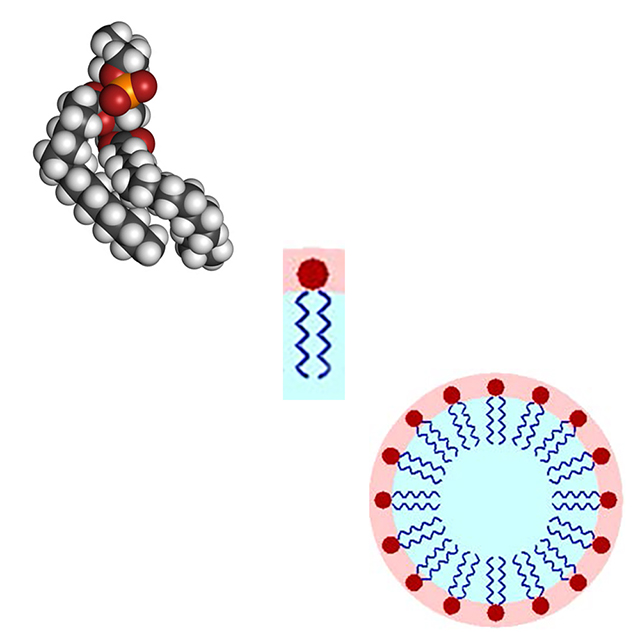
Remember also from Unit 2 that surfactants act like soap, breaking up hydrogen bonds and reducing surface tension. In the lungs, surfactant is manufactured by type II alveolar cells. Surfactant acts to break up surface tension caused by water molecules in the airliquid interface within the alveoli of the lungs.
Surfactant is necessary to prevent the collapse of alveoli on exhalation. Amounts of surfactant sufficient to permit survival of a premature infant are not produced until 26-28 weeks of gestation.
The important role of surfactant in infant respiratory distress syndrome was discovered in the 1950s. After several decades of research, an artificial surfactant was developed. This is administered into the airway of the infant at, or shortly after birth. Immediate improvements in lung function are usually observed. Infant mortality has greatly decreased since the advent of exogenous surfactant therapy.
Media Attributions
- U17-064 Development of the Lower Respiratory System © Betts, J. Gordon; Young, Kelly A.; Wise, James A.; Johnson, Eddie; Poe, Brandon; Kruse, Dean H. Korol, Oksana; Johnson, Jody E.; Womble, Mark & DeSaix, Peter is licensed under a CC BY (Attribution) license
- U17-065 Development of Lungs Table © Hutchins, Jim is licensed under a CC BY-SA (Attribution ShareAlike) license
- U17-066 Surface Tension © Crookston, Alexa is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
- U17-027a Structure of an Alveolus © Cornelius, Emma is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
- U17-067 dipalmitoylphosphatidylcholine pulmonary surfactant © PubChem is licensed under a CC0 (Creative Commons Zero) license
- U17-068 Surfactant Micelle Structure © Gilbert, Stephen and PubChem adapted by Jim Hutchins is licensed under a CC BY-SA (Attribution ShareAlike) license

{kind=link}