Hormones of the Anterior Pituitary
Objective 5
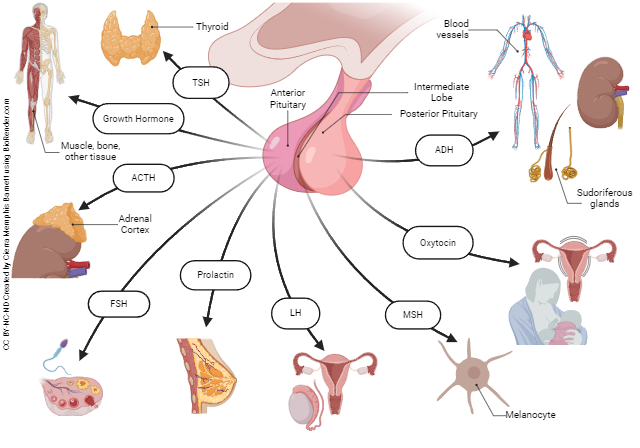
List the hormones of the adenohypophysis, their target organs, their principal actions, and the correlating releasing-hormone from the hypothalamus. Identify the anterior pituitary cells that produce each hormone.
Remember from Objective 3 that there is a chain of events that eventually cause a hormone from the adenohypophysis to target a cell or gland. That chain of events starts with a releasing hormone from the hypothalamus. This releasing hormone travels through blood vessels (hypophyseal portal veins) to the anterior pituitary where target cells release their hormone. In the next chain of events, the anterior pituitary hormone targets cells with receptors for that hormone. Inhibiting hormones may also be released that suppress the release of the hormone. For example, if growth hormone is high, the hypothalamus releases growth hormone inhibiting hormone (GHIH) to suppress the release of growth hormone.
In the following table, inhibiting hormones are listed in the first column. For mapping out the pathway of a particular hormone, start with the hypothalamic releasing hormone in the second column. This will then release the anterior pituitary hormone (3rd column). The targets and function of the hormone are listed in the last column.
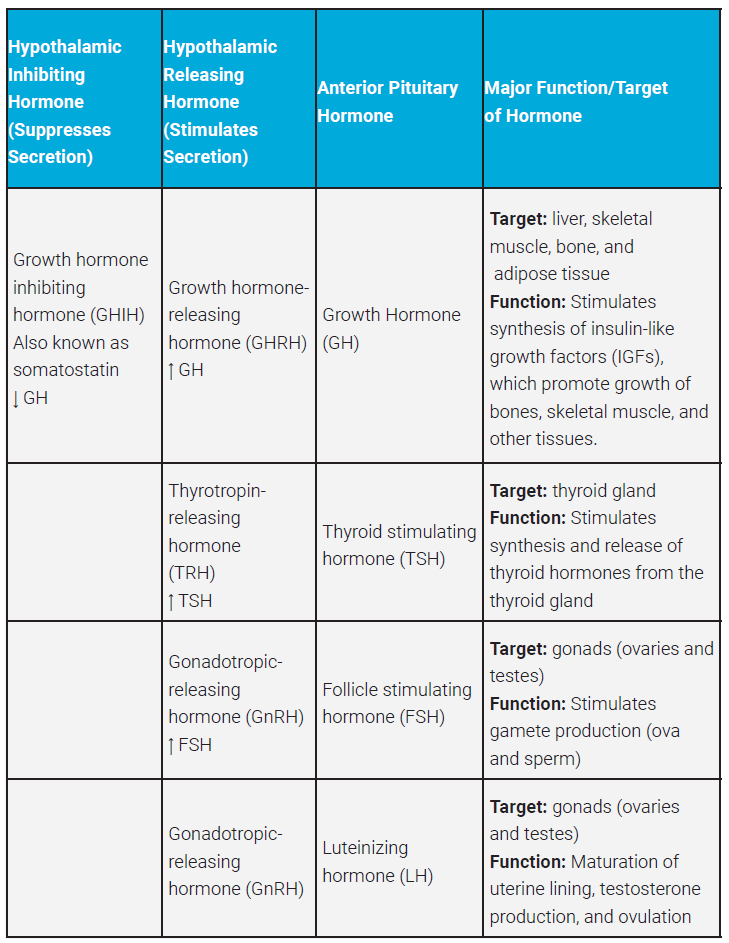
Hypothalamic-Pituitary Hormones & Their Effects
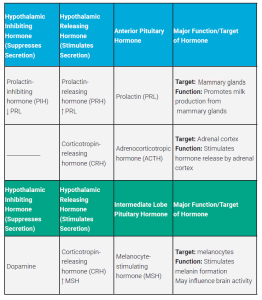
As a point of interest, you may be wondering how CRH stimulates both ACTH and MSH in the pituitary. Corticotropic cells produce the prohormone propriomelanocortin (POMC). Cleavage of POMC occurs in hormone synthesizing cells. POMC may be cleaved to ACTH, which can be further broken down to MSH. Therefore, the take home message is both ACTH and MSH come from the same prohormone.
You may have noticed that hormones from the hypothalamus that trigger the release of anterior pituitary hormones are all called releasing hormones. The hypothalamus may also inhibit the release of anterior pituitary hormones by secreting inhibiting hormones. When the anterior pituitary secretes a hormone that acts on another endocrine gland we call this a tropic hormone. For example, thyroid stimulating hormone (TSH) targets the thyroid gland, a true endocrine gland because its sole function is to release hormone. TSH by definition then, is a tropic hormone.
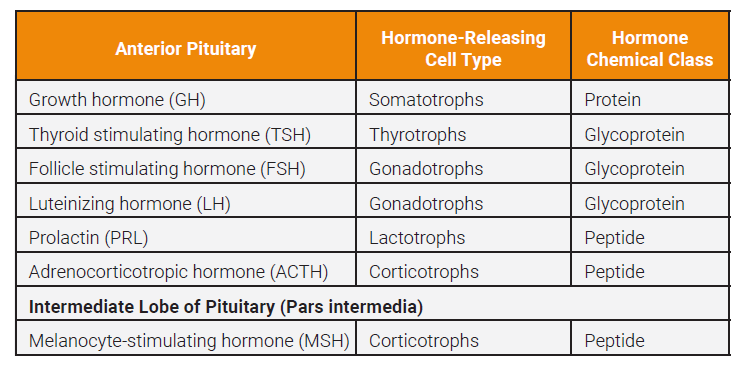
Each anterior pituitary hormone has its own special cells producing this hormone. The following chart shows the cells that produce and secrete each hormone, and the chemical class of the hormone.
Character of Anterior Pituitary Hormones
Now let’s explore a little further some of the anterior pituitary hormones.
Growth Hormone
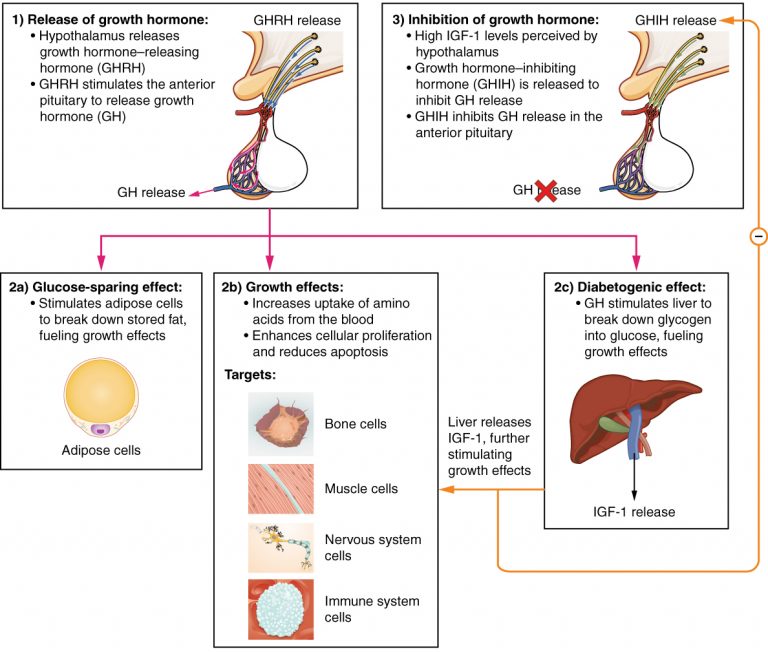
Growth hormone (GH or hGH), also called somatotropin, regulates the growth of the human body, protein synthesis, and cellular replication. GH’s primary function is anabolic; it promotes protein synthesis and tissue building through direct and indirect mechanisms. Growth hormone releasing hormone (GHRH) from the hypothalamus triggers the release of GH. GH stimulates adipose cells to break down stored fat releasing it as energy used for growth. GH also increases the uptake of amino acids from the blood and causes cell division. GH stimulates increased glucose for energy by stimulating the liver to break down glycogen stores. GH also causes the liver to secrete insulin like growth factor-1, which further stimulates growth and, as the name applies, acts like insulin in facilitating the uptake of glucose by cells.
Elevated levels of IGF-1 trigger the hypothalamus to release growth hormone-inhibiting hormone (GHIH), also a neurotransmitter known as somatostatin, which then inhibits further release of more growth hormone. Notice the negative feedback loop in this illustration of the actions of growth hormone.
Clinical Connection
 Hormone disorders are caused by having too much or too little of the hormone in question. In disorders of GH, we have to consider if the individual is a child or an adult. Hyposecretion of GH during childhood may lead to pituitary dwarfism. The individual has normal body proportions but does not reach normal height. All of the body systems may be affected.
Hormone disorders are caused by having too much or too little of the hormone in question. In disorders of GH, we have to consider if the individual is a child or an adult. Hyposecretion of GH during childhood may lead to pituitary dwarfism. The individual has normal body proportions but does not reach normal height. All of the body systems may be affected.
Too much growth hormone during childhood leads to giantism. Overall body proportions will remain consistent, but the patient will be very tall. The main cause of giantism is a tumor of the anterior pituitary.
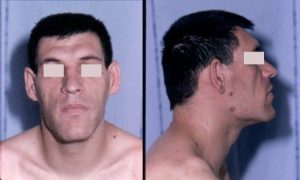 You might ask what happens if there is too much GH in an adult. A condition called acromegaly may result. While long bones are closed, bones may become thicker and denser and tissues may enlarge. Soft tissue may enlarge with possible nerve entrapment.
You might ask what happens if there is too much GH in an adult. A condition called acromegaly may result. While long bones are closed, bones may become thicker and denser and tissues may enlarge. Soft tissue may enlarge with possible nerve entrapment.
Human growth hormone has been implicated in doping in sports1. An artificial form was made in the early 1990s. This form is hard to differentiate from normal growth hormone, and thus is hard to detect. It’s popular because of its anabolic effect on muscle growth and supposed performance-enhancing ability. The illicit use of GH is often combined with anabolic steroids so it’s difficult to determine if it really enhances athletic ability. Side effects may include acromegaly with swelling of the hands and feet, fluid retention, excessive sweating as well as enlargement of the heart, osteoporosis, menstrual irregularities, and impotence1. That last side effect may deter even the most determined athlete!
Thyroid Stimulating Hormone
Thyroid gland activity is regulated by thyroid-stimulating hormone (TSH) which is released when the hypothalamus releases thyrotropin-releasing hormone (TRH). When TSH stimulates the thyroid gland, the thyroid hormones triiodothyronine (T3) and thyroxine (T4) are released. Elevated levels of thyroid hormones suppress TRH in a negative feedback loop. We will discuss the thyroid gland in Objective 6.
Adrenocorticotropic Hormone
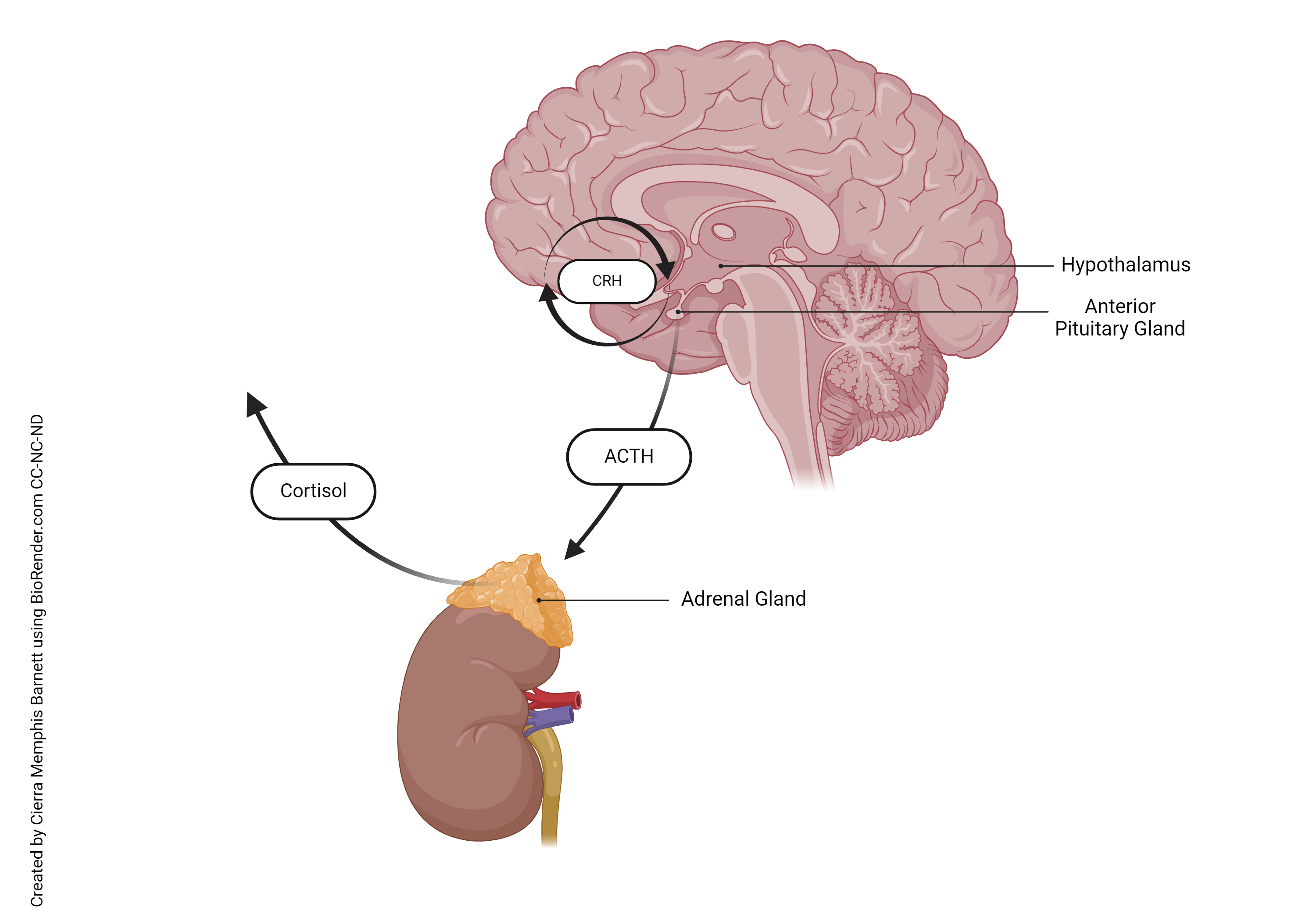 Corticotropin-releasing hormone stimulates the release of adrenocorticotropic hormone (ACTH) from the anterior pituitary. This hormone, as illustrated earlier, then targets the adrenal cortex (cortex means bark or the superficial region of the adrenal glands). The adrenals release several hormones, including cortisol, that will be further studied in Objective 8.
Corticotropin-releasing hormone stimulates the release of adrenocorticotropic hormone (ACTH) from the anterior pituitary. This hormone, as illustrated earlier, then targets the adrenal cortex (cortex means bark or the superficial region of the adrenal glands). The adrenals release several hormones, including cortisol, that will be further studied in Objective 8.
Follicle-Stimulating Hormone & Luteinizing Hormone
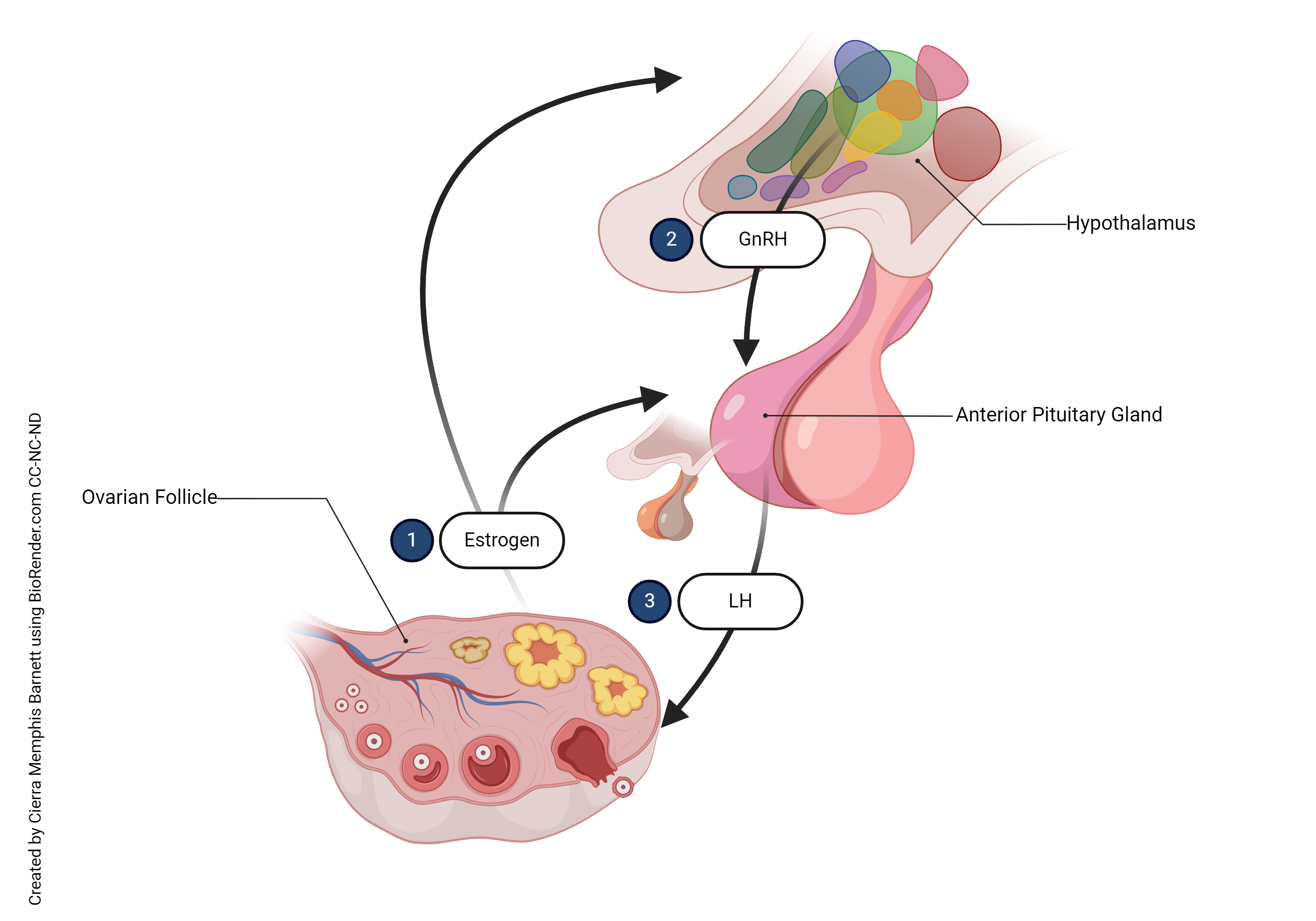 Many hormones regulate the reproductive system in both males and females. These hormones will be studied further in the reproductive system. For now, we will introduce two hormones stimulated by the release of gonadotropin-releasing hormone (GnRH) from the hypothalamus. The mad rush of hormones initiating puberty is started by the release of GnRH. Follicle-stimulating hormone (FSH) stimulates the development of the gametes: ova (eggs) in females and sperm in males. A surge of luteinizing hormone (LH) triggers ovulation in women and also triggers the production of estrogen and progesterone in the ovaries. In males, LH stimulates the production of testosterone in the male testes.
Many hormones regulate the reproductive system in both males and females. These hormones will be studied further in the reproductive system. For now, we will introduce two hormones stimulated by the release of gonadotropin-releasing hormone (GnRH) from the hypothalamus. The mad rush of hormones initiating puberty is started by the release of GnRH. Follicle-stimulating hormone (FSH) stimulates the development of the gametes: ova (eggs) in females and sperm in males. A surge of luteinizing hormone (LH) triggers ovulation in women and also triggers the production of estrogen and progesterone in the ovaries. In males, LH stimulates the production of testosterone in the male testes.
Prolactin (PRL)
Just as the name implies, prolactin promotes milk production (lactation) in women. Prolactin needs a lot of help. Other hormones that have a permissive effect with prolactin must prime mammary glands. These hormones include estrogens, progesterone, glucocorticoids, growth hormone, thyroxine, and insulin. Wow, it takes a lot to produce milk! The level of prolactin rises during pregnancy leading to the development of the mammary glands, and after birth, to milk production. When a woman is not pregnant, prolactin-inhibiting hormone suppresses prolactin. The role of prolactin in males is not well known although studies have shown an interdependence between testosterone and prolactin. In vivo, prolactin has been shown to upregulate the synthesis of testosterone, demonstrating that it is an important hormone in regulating male fertility2.
Melanocyte-Stimulating Hormone
Corticotropin-releasing hormone from the hypothalamus also stimulates the release of melanocyte-stimulating hormone (MSH). As mentioned earlier, this hormone is made in the intermediate pituitary, located between the anterior and posterior pituitary. This hormone stimulates melanin production and secretion by melanocytes. In the skin, MSH can be triggered by exposure to UV light (why you get tan if you lay out in the sun). MSH from the pituitary is a little more complicated. MSH can trigger increased melanin production in individuals with darker skin, even though the amount of melanocytes are about the same. MSH production may increase during pregnancy. Combined with estrogens, this may cause darkening of the skin, especially around the areolas and the labia minora. Dopamine, from the hypothalamus, inhibits the production and release of MSH.
Clinical Connection
 In Addison’s disease, the adrenal cortex is damaged and doesn’t produce enough hormone. The hypothalamus responds by producing more CRH. We’ve already learned that CRH targets the release of MSH in addition to ACTH. MSH targets melanocytes to produce more pigment. Because of this, patients with Addison’s disease often experience some hyperpigmentation, a result of the excess production of MSH.
In Addison’s disease, the adrenal cortex is damaged and doesn’t produce enough hormone. The hypothalamus responds by producing more CRH. We’ve already learned that CRH targets the release of MSH in addition to ACTH. MSH targets melanocytes to produce more pigment. Because of this, patients with Addison’s disease often experience some hyperpigmentation, a result of the excess production of MSH.
Footnotes
- Saugy, M., Robinson, N., Saudan, C., Baume, N., Avois, L., & Mangin, P. (2006). Human growth hormone doping in sport. British journal of
sports medicine, 40 Suppl 1(Suppl 1), i35–i39. https://doi.org/10.1136/bjsm.2006.027573 - Gill-Sharma M. K. (2009). Prolactin and male fertility: the long and short feedback regulation. International journal of endocrinology, 2009, 687259. https://doi.org/10.1155/2009/687259
Media Attributions
- U14-020 Table of Anterior Pituitary Hormones part 1 © Newton, Kathy is licensed under a CC BY-SA (Attribution ShareAlike) license
- U14-021-table-of-anterior-pituitary-hormones-part-2 edited (1) © Jim Hutchins is licensed under a CC BY-SA (Attribution ShareAlike) license
- U14-022 Table of Anterior Pituitary Hormone Releasing Cell Type and Chemical Class © Newton, Kathy is licensed under a CC BY-SA (Attribution ShareAlike) license
- U14-023 Hormonal Regulation of Growth © Betts, J. Gordon; Young, Kelly A.; Wise, James A.; Johnson, Eddie; Poe, Brandon; Kruse, Dean H. Korol, Oksana; Johnson, Jody E.; Womble, Mark & DeSaix, Peter is licensed under a CC BY (Attribution) license
- U14-024 Giant and a Dwarf © Wellcome Collection is licensed under a CC BY (Attribution) license
- U14-025 Facial Aspect of a Patient with Acromegaly © Chanson, Phillipe and Salenave, Sylvie is licensed under a CC BY (Attribution) license
- U14-026b ACTH’s Impact on Cortisol © Barnett, Cierra Memphis is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
- U14-027a Hormonal Control of Ovulation © Barnett, Cierra Memphis is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license
- U14-026a Addison’s Legs © Heilman, James MD is licensed under a CC BY-SA (Attribution ShareAlike) license
- U14-027b Organs Impacted by Hormones from the Pituitary © Barnett, Cierra Memphis is licensed under a CC BY-NC-ND (Attribution NonCommercial NoDerivatives) license

{kind=link}