Lateral Medullary Syndrome (Wallenberg Syndrome)
Brooke Hildt and Jim Hutchins
Overview
Wallenberg syndrome, also known as lateral medullary syndrome or posterior inferior cerebellar artery syndrome, is a neurological condition that results in damage to part of the brain stem. This damage can result from restricted blood flow due to artery damage or from a stroke.
https://radiopaedia.org/articles/lateral-medullary-syndrome?lang=us
1/5 strokes in posterior circulation
lateral medullary syndrome is the most common of the posterior circulation strokes
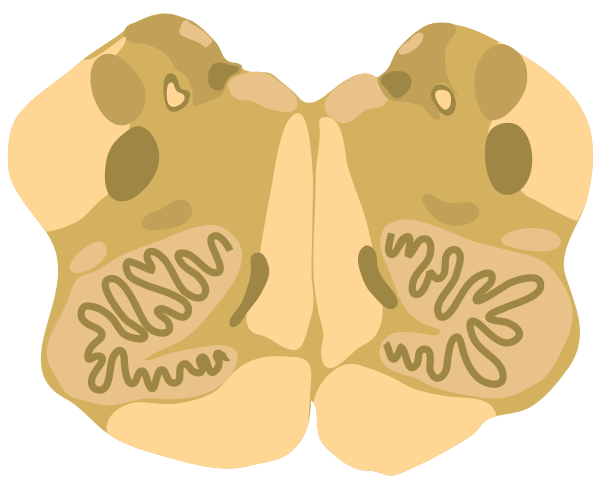
Structures affected
- inferior cerebellar peduncle
- dorsolateral medulla
- descending spinal tract
- nucleus of the V nerve
- vagus nerve and nucleus
- glossopharyngeal nerve and nucleus
- descending sympathetic fibers
Signs and Symptoms
- vestibulocerebellar symptoms
- ipsilateral hemiataxia
- vertigo
- falling toward side of lesion
- multidirectional nystagmus (inferior cerebellar peduncle and vestibular nucleus)
- autonomics
- ipsilateral Horner syndrome
- hiccups
- sensory
- loss of p&t over ipsilateral face & contralateral body
- bulbar
- hoarseness
- dysphonia
- dysphagia
- dysarthria
- decreased gag reflex (nucleus ambiguus)
Diagnosis
Diagnosis of Wallenberg Syndrome includes a clinical examination, patient history, MRI with diffusion-weighted imaging, angiogram, and/or an EKG.
Treatment
Treatment will vary based on the cause of Wallenberg Syndrome. Possible treatment interventions include IV administration of thrombolytic drugs, surgery to remove clots/ repair a damaged artery, and possible long-term rehabilitative therapies.
Risk Factors
- Hypertension
- Smoking
- Diabetes
- Neck injuries
Case Study
49-year-old female presenting with sudden onset right hemicranial headache that woke her from sleep around 4am this morning. Reported 6/10 pain over the right occipital region, dizziness, and a numb/tingling sensation over her right side of her face. Also developed choking sensation and severe bouts of cough when trying to drink water. One hour after presentation, she experienced difficulty speaking and developed partial closing of her right eyelid.
Personal and family history were unremarkable. On clinical examination, she was unable to speak but could understand spoken words and follow verbal commands with normal vitals and behavior. Muscle tone and power were normal in all four limbs. Pupils were round and reactive to light. Impaired tough, temperature, and pain on the R side. Partial R ptosis.
Clinical diagnosis of posterior circulation stroke was confirmed with MRI. MR angiography of brain was suggestive of irregular narrowing of R vertebral artery. Electrocardiogram showed normal sinus rhythm.
Patient was treated with dual-antiplatelet therapy (aspirin and clopidogrel) and high-dose statin. Ryle’s tube was placed for enteral feeding along with neurorehabilitation for dysphagia and dysarthria. Vertigo managed with betahistine and ondansetron. Patient made good recovery and was able to walk unassisted upon discharge 1 week after presentation.
Media Attributions
- Medulla_-_Middle_level_cross_section.svg © Kevin Dufendach is licensed under a CC BY-SA (Attribution ShareAlike) license

{kind=link}